Research Article
Evaluation of Horizontal Lip Position in Adults with Different Skeletal Patterns: A Cephalometric Study

Vinay V Umale1, Kamlesh Singh2, Aftab Azam3, Madhvi Bhardwaj4 and Rohit Kulshrestha5*
1Post Graduate Student, Department of Orthodontics and Dentofacial Orthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
2Professor, Department of Orthodontics and Dentofacial Orthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
3Reader, Department of Orthodontics and Dentofacial Orthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
4Reader, Department of Orthodontics and Dentofacial Orthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
5Post Graduate Student, Department of Orthodontics and Dentofacial Orthopedics, Saraswati Dental College, Lucknow, Uttar Pradesh, India
*Address for Correspondence: Dr. Rohit Kulshrestha, Post Graduate Student, Department of Orthodontics and Dentofacial Orthopedics, Room no. 3, PG Boys Hostel, Saraswati Dental College, Lucknow, Uttar Pradesh, India, Email: [email protected]
Dates: Submitted: 28 February 2017; Approved: 09 March 2017; Published: 10 March 2017
How to cite this article: Umale VV, Singh K, Azam A, Bhardwaj M, Rohit K. Evaluation of Horizontal Lip Position in Adults with Different Skeletal Patterns: A Cephalometric Study. J Oral Health Craniofac Sci. 2017; 2: 009-016. DOI: 10.29328/journal.johcs.1001005
Copyright License: 2017 Umale VV, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Lip analysis; Soft tissue evaluation; Holdaways angle
ABSTRACT
Aim: To evaluate sexual dimorphism in horizontal lip position in adults with different skeletal patterns.
Material and Methods: The sample comprised of 120 patients (Females 18 years and above, Males 21 years and above) with no history of previous orthodontic treatment or functional jaw orthopaedic treatment. They were divided into different groups based on the ANB angle and gender. Group I and II included 30 males and 30 females with skeletal class I malocclusion (ANB 0-4 degree). Group III and IV included 30 males and 30 females with skeletal class II malocclusion respectively (ANB above 4 degree).
Results: When comparison between males and females (Class I+Class II) was done S-line (p<0.001), B-line (p<0.001), E-line (p<0.001), Holdaways angle (p<0.001) and Merrifield angle (p<0.001) were found to be statistically significant. S-line (p<0.001), E-line (p<0.001) and Holdaways angle (p<0.001) were found to be statistically significant when comparison was done between males and females (Class I). When comparison was done between males and females (Class II) only Holdaways angle (p<0.001) showed a significant statistical difference.
Conclusion: Sexual dimorphism was found in various lip parameters. Significant amount of differences were found between Class I and Class II (male and female) subjects.
INTRODUCTION
Facial beauty is assessed by the balance between soft and hard tissues which are seen on the face and head region i.e. fore head, orbits, zygoma, nose, lips, chin and throat. Due to this many investigators have tried to study the relationship between these structures with growing interest. Unattractive facial proportions can be changed or modified by using various techniques namely dentofacial orthopaedics, orthognathic surgery, and aesthetic soft tissue surgery. Rhinoplasty, lip lifting, lip augmentation, and cheek augmentation are some procedures that can further improve the patient’s overall aesthetics and at the same time bring them closer to better facial harmony without any changes in occlusal characteristics [1].
Facial balance or harmony generally is determined by comparisons made between morphological relationships of hard tissues and proportions between the soft tissues namely nose, lips, and chin. It is necessary for the orthodontist to have knowledge about the amount, direction and rate of growth expected in these soft tissue facial structures. Many authors have mentioned the importance of taking into consideration both growth and treatment in predicting post-orthodontic facial changes [2]. The outlook of beauty has changed over the years and differs from one population to another, it has been a thing of importance to people of all cultures. Investigators have developed numerous methods of analysis to deduce the diagnostic information from the lateral cephalograms. For a long time, orthodontists have focused on the position, size and fullness of the lip as the most important features in determining beauty. Several lines and parameters have been introduced to assess the antero-posterior position of the upper and lower lips and the aesthetic quality of the profile. Steiner [3] evaluated the soft tissue profile by connecting a line (S line) from the middle of the S-shaped curve between the tip of the nose and sub-nasale to the soft tissue pogonion and mentioned that the lips should touch the reference line. Lip analysis done by Rickett’s [4] consists of a line E-line (Esthetic line) which is drawn from the tip of the nose to soft tissue pogonion on the chin. Ricketts mentioned that the lips lie behind this E-line at a mean distance of 4 mm for the upper and 2 mm for the lower lip respectively. Burstone’s [5] B line was drawn from soft tissue sub-nasale to soft tissue pogonion. He stated that the lips were positioned anterior to this line at a mean distance of 3.5mm for the upper and 2.2 mm for the lower lip respectively.
Holdaway’s [6] soft tissue analysis describes using the H line (Harmony line) which is drawn to tangent to the upper lip from soft tissue pogonion. His results showed that the angle formed between nasion-point B line and the Harmony line should be 7° to 8° when the ANB angle was between 1° to 3° and the lower lip was on the H line. The tip of the nose was 9 mm anterior to this reference line. Merrifield modified Holdaway’s Harmony line and named it the Z angle (line drawn from soft tissue pogonion to the most forwardly placed lip), and measured this Z angle with the Frankfort Horizontal plane. It was 80° in adults. A line (S2 line) drawn from soft tissue nasion to soft tissue pogonion was developed by Sushner [7]. He stated that the upper and lower lips were located in front of this line in the black population. Along with the studies stated above, cephalometric norms for different ethnic and racial groups have been developed. All these studies show that normal measurements for one ethnic group should not be considered ideal for every race or ethnic group. Different racial groups should be treated according to their own characteristics. Thus the aim of this study was to evaluate variations in horizontal lip position in male and female adults with class I and class II skeletal malocclusions.
MATERIAL AND METHODS
Pre-treatment lateral cephalograms of 120 patients who reported to the Department of Orthodontics Saraswati Dental College Lucknow for orthodontic treatment were chosen for the study. Written consent forms were taken from each of the patients after being informed about the nature of the study in detail. The study was approved by the local Ethical Committee of Saraswati Dental College and Hospital Lucknow Each subject met the following inclusion criteria:
• 18 years above females and 21 years above males.
• No history of previous orthodontic treatment or functional jaw orthopaedic treatment.
• No history of any surgery involving the jaws, cleft lip and palate and any systemic disease affecting normal growth.
• No previous history of trauma to the dentofacial structures.
Based on the ANB angle and gender, all the subjects were divided into following four groups:
• Group I included 30 males with skeletal class I malocclusion (ANB 0-4 degree)
• Group II included 30 females with skeletal class I malocclusion (ANB 0-4 degree).
• Group III included 30 males with skeletal class II malocclusion (ANB above 4 degree).
• Group IV included 30 females with skeletal class II malocclusion (ANB above 4 degree).
Lateral cephalograms were taken in standing position with the Frankfort Horizontal plane parallel to the floor. All the cephalograms were recorded with the same exposure parameters (KvP-80, mA-10, exposure time 0.5 sec) with the same magnification and the same machine (Kodak 8000C Digital and Panoramic System Cephalometer Rochester, NY, USA). The x-rays were printed using Fujifilm Medical Dry Imaging film (8 X 10 inches in size) and the Fujifilm Dry pix plus printer. All cephalograms were traced manually using lead acetate paper and 4B tracings pencils by the same operator. Various landmarks were identified, angular and linear measurements were measured.
The following cephalometric landmarks were used to assess the lip parameters (Figure 1).
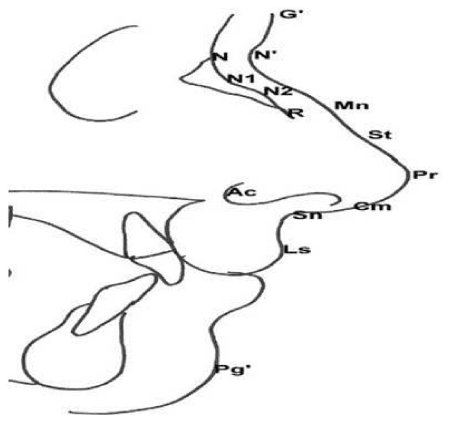
Figure 1: Lateral cephalometric landmarks used to assess the lip.
1. Glabella (G’): the most prominent soft tissue point of the frontal bone.
2. Soft-tissue nasion (N’): the point of greatest concavity in the mid-line between the fore-head and the nose.
3. Midnasale (Mn): the halfway point on nasal length (N’-Pr) that divides the dorsum into upper and lower dorsum.
5. Nasion (N): the intersection of the frontal and nasal bones.
9. Pronasale (Pr): the tip of nose (nasal tip).
11. Subnasale (Sn): the point at which the columella merges with the upper lip in the mid-sagittal plane.
12. Alar curvature point (Ac): is the most visible convex point on the nasal alar curvature.
13. Labrale superior (Ls): is the point on the mucocutanous border of the upper lip.
14. Labrale Inferior (Li): the point indicating the mucocutanous border of the lower lip.
15. Soft tissue pogonion (Pg’): the most anterior point on the chin in the mid sagittal plane.
The following reference planes were used to assess the lip position (Figure 2).
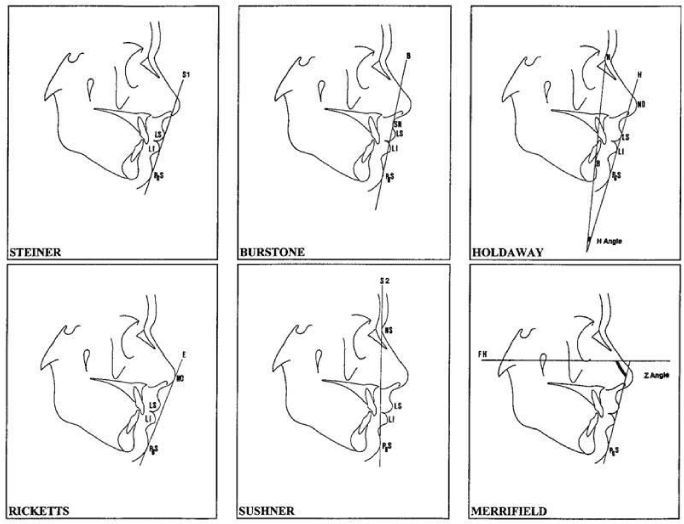
Figure 2: Reference planes and variables were used to assess the lip position.
1. Steiner’s S1- line from the middle of the S shaped curvature between the tip of the nose and sub-nasale to the soft tissue pogonion.
2. Rickett’s E- is the line drawn from the tip of the nose to the soft tissue pogonion.
3. Burstone’s B- line was drawn from soft tissue sub-nasale to soft tissue pogonion.
4. Sushner’s S2- line drawn from soft tissue nasion to soft tissue pogonion.
5. Holdaway’s H- line is drawn tangent to the upper lip from soft tissue pogonion. ‘H’ line angle is taken between the nasion-point B line and H line.
6. Merrifield ‘Z’ angle is taken between a line from soft tissue pogonion to the most procumbent lip, and the Frankfort horizontal plane.
STATISTICAL ANALYSIS
A master file was created, and the data was analyzed statistically on a computer with Statistical Package for Social Sciences (SPSS) software (version 13). A data file was made under dBase and converted into a micro stat file. The data was subjected to descriptive analysis for mean, range, standard deviation and 95% confidence interval. Group differences were analyzed with one-way analysis of variance (ANOVA). For many comparisons, a post hoc Tukey honestly significant difference (HSD) test was used. To identify errors due to radiographic measurements, 12 radiographs were selected randomly. Their tracings and measurements were repeated 6 weeks after the first measurements were taken. A paired sample t-test was applied to the first and second measurements, the differences between measurements were insignificant.
RESULTS
S-line (p<0.001), E-line (p<0.001) and Holdaways angle (p<0.001) were found statistically significant when comparison was done between males and females (Class I) (Table 1). When comparison was done between males and females (Class II) only Holdaways angle (p<0.001) showed a significant statistical difference (Table 2). E-line (p<0.001) showed a statistical difference when comparison was done between males and females gender (Class I+Class II) (Table 3). When comparison between males and females (Class I+Class II) was done S-line (p<0.001), B-line (p<0.001), E-line (p<0.001), Holdaways angle (p<0.001) and Merrifield angle (p<0.001) were statistically significant (Table 4).
| Table 1: Descriptive statistics of males and females and comparison of sex differences in dentally normal group (Class I). | |||||||||||
| SN | Variable | Male (n=30) | Female (n=30) | "t" | "p" | ||||||
| Mean | SD | Min | Max | Mean | SD | Min | Max | ||||
| 1 | S1 line upper lip(mm) | 1.43 | 2.31 | -3.5 | 6 | 2.83 | 2.57 | -2 | 9 | -2.215 | 0.031 |
| 2 | S1 line lower lip(mm) | 2.17 | 2.78 | -3 | 10 | 3.60 | 3.33 | -2 | 10 | -1.811 | 0.075 |
| 3 | E line upper lip (mm) | -2.50 | 3.42 | -11 | 3 | -0.37 | 3.09 | -6 | 5 | -2.535 | 0.014 |
| 4 | E line lower lip (mm) | -0.08 | 3.43 | -7 | 7 | 2.07 | 3.68 | -4 | 8 | -2.342 | 0.023 |
| 5 | B line upper lip (mm) | 4.95 | 2.17 | 0 | 10 | 5.87 | 2.16 | 2 | 10.00 | -1.640 | 0.106 |
| 6 | B line lower lip (mm) | 4.35 | 2.29 | 0 | 12 | 5.37 | 2.92 | 1 | 11 | -1.501 | 0.139 |
| 7 | S2 line upper lip (mm) | 11.75 | 3.39 | 3.5 | 18 | 11.60 | 3.32 | 5 | 19 | 0.173 | 0.863 |
| 8 | S2 line lower lip (mm) | 8.53 | 3.13 | 1 | 15.5 | 8.50 | 3.37 | 3 | 14 | 0.040 | 0.968 |
| 9 | Holdaway angle | 14.60 | 4.90 | 2 | 23 | 17.40 | 5.76 | 8 | 36 | -2.028 | 0.047 |
| 10 | Merriefield angle | 65.93 | 10.28 | 40 | 85 | 61.93 | 13.00 | 30 | 84 | 1.322 | 0.191 |
| SD - Standard Deviation, "t"- degree of variation, p=0.05 value of significance | |||||||||||
| Table 2: Descriptive statistics of males and females and comparison of sex differences in malocclusion group (Class II). | |||||||||||
| SN | Variable | Male (n=30) | Female (n=30) | "t" | "p" | ||||||
| Mean | SD | Min | Max | Mean | SD | Min | Max | ||||
| 1 | S1 line upper lip(mm) | 4.12 | 2.18 | -1 | 9 | 3.70 | 2.03 | 0 | 7 | 0.766 | 0.447 |
| 2 | S1 line lower lip(mm) | 4.47 | 2.68 | 1 | 11 | 5.00 | 3.14 | -2 | 11 | -0.707 | 0.482 |
| 3 | E line upper lip (mm) | 0.78 | 2.42 | -5 | 7 | 0.90 | 2.32 | -4 | 5 | -0.191 | 0.850 |
| 4 | E line lower lip (mm) | 2.75 | 2.87 | -1.5 | 9 | 3.50 | 3.08 | -3 | 10 | -0.975 | 0.334 |
| 5 | B line upper lip (mm) | 6.95 | 2.00 | 1 | 11 | 6.35 | 1.76 | 3 | 9.00 | 1.232 | 0.223 |
| 6 | B line upper lip (mm) | 6.18 | 2.71 | 3 | 13 | 6.57 | 2.81 | 1 | 12 | -0.538 | 0.593 |
| 7 | S2 line upper lip (mm) | 16.17 | 2.73 | 11 | 21 | 14.88 | 2.75 | 9 | 19 | 1.815 | 0.075 |
| 8 | S2 line lower lip (mm) | 10.70 | 3.09 | 7 | 19 | 10.92 | 2.93 | 4 | 17.5 | -0.279 | 0.781 |
| 9 | Holdaway angle | 21.73 | 4.43 | 12 | 36 | 19.43 | 3.52 | 12 | 26 | 2.225 | 0.030 |
| 10 | Merriefield angle | 54.37 | 8.73 | 34 | 69 | 53.63 | 9.69 | 39 | 72 | 0.308 | 0.759 |
| SD - Standard Deviation, "t"- degree of variation, p=0.05 value of significance | |||||||||||
| Table 3: Descriptive statistics of males and females and comparison of sex differences (Class I+Class II). | |||||||||||
| SN | Variable | Male (n=60) | Female (n=60) | "t" | "p" | ||||||
| Mean | SD | Min | Max | Mean | SD | Min | Max | ||||
| 1 | S1 line upper lip(mm) | 2.78 | 2.61 | -3.5 | 9 | 3.27 | 2.34 | -2 | 9 | -1.087 | 0.279 |
| 2 | S1 line lower lip(mm) | 3.32 | 2.94 | -3 | 11 | 4.30 | 3.29 | -2 | 11 | -1.726 | 0.087 |
| 3 | E line upper lip (mm) | -0.86 | 3.37 | -11 | 7 | 0.27 | 2.79 | -6 | 5 | -1.993 | 0.049 |
| 4 | E line lower lip (mm) | 1.33 | 3.45 | -7 | 9 | 2.78 | 3.44 | -4 | 10 | -2.307 | 0.023 |
| 5 | B line upper lip (mm) | 5.95 | 2.30 | 0 | 11 | 6.11 | 1.97 | 2 | 10.00 | -0.405 | 0.686 |
| 6 | B line lower lip (mm) | 5.27 | 2.65 | 0 | 13 | 5.97 | 2.91 | 1 | 12 | -1.379 | 0.171 |
| 7 | S2 line upper lip (mm) | 13.96 | 3.78 | 3.5 | 21 | 13.24 | 3.44 | 5 | 19 | 1.086 | 0.280 |
| 8 | S2 line lower lip (mm) | 9.62 | 3.27 | 1 | 19 | 9.71 | 3.36 | 3 | 17.5 | -0.151 | 0.880 |
| 9 | Holdaway angle | 18.17 | 5.86 | 2 | 36 | 18.42 | 4.84 | 8 | 36 | -0.255 | 0.799 |
| 10 | Merriefield angle | 60.15 | 11.11 | 34 | 85 | 57.78 | 12.11 | 30 | 84 | 1.115 | 0.267 |
| SD - Standard Deviation, "t"- degree of variation, p=0.05 value of significance | |||||||||||
| Table 4: Descriptive statistics of Class I and Class II and comparison of Class differences (Both Genders). | |||||||||||
| SN | Variable | Class 1 (n=60) | Class 2 (n=60) | "t" | "p" | ||||||
| Mean | SD | Min | Max | Mean | SD | Min | Max | ||||
| 1 | S1 line upper lip(mm) | 2.13 | 2.53 | -3.5 | 9 | 3.91 | 2.10 | -1 | 9 | -4.184 | <0.001 |
| 2 | S1 line lower lip(mm) | 2.88 | 3.12 | -3 | 10 | 4.73 | 2.91 | -2 | 11 | -3.357 | 0.001 |
| 3 | E line upper lip (mm) | -1.43 | 3.41 | -11 | 5 | 0.84 | 2.35 | -5 | 7 | -4.258 | <0.001 |
| 4 | E line lower lip (mm) | 0.99 | 3.69 | -7 | 8 | 3.13 | 2.98 | -3 | 10 | -3.486 | 0.001 |
| 5 | B line upper lip (mm) | 5.41 | 2.19 | 0 | 10 | 6.65 | 1.89 | 1 | 11.00 | -3.318 | 0.001 |
| 6 | B line upper lip (mm) | 4.86 | 2.65 | 0 | 12 | 6.38 | 2.74 | 1 | 13 | -3.080 | 0.003 |
| 7 | S2 line upper lip (mm) | 11.68 | 3.33 | 3.5 | 19 | 15.53 | 2.79 | 9 | 21 | -6.867 | <0.001 |
| 8 | S2 line lower lip (mm) | 8.52 | 3.23 | 1 | 15.5 | 10.81 | 2.99 | 4 | 19 | -4.037 | <0.001 |
| 9 | Holdaway angle | 16.00 | 5.49 | 2 | 36 | 20.58 | 4.13 | 12 | 36 | -5.168 | <0.001 |
| 10 | Merriefield angle | 63.93 | 11.79 | 30 | 85 | 54.00 | 9.15 | 34 | 72 | 5.154 | <0.001 |
| SD - Standard Deviation, "t"- degree of variation, p=0.05 value of significance | |||||||||||
DISCUSSION
Achieving an aesthetic change in the soft tissue profile after orthodontic treatment often is one of the main concerns of the orthodontic patient. The perception of beauty varies widely among all individuals of different races and ethnic groups. Different authors have tried to quantify objectively their norms and ideas of the ideal soft tissue profile [8-12]. The quantification and expression of the soft tissue profile is not easy because of the diversity in races and also due to the profile which as seen on the lateral cephalogram, consists of many curved lines.
Present study evaluated horizontal lip position using Steiner’s S line, Ricketts E line, Burstone’s B line, Sushner’s line, Holdaway H angle and Merrifield’s Z angle. McNamara et al. [13] evaluated the position of the lips with the soft tissue analysis of Steiner, Holdaway’s and Rickett’s on Caucasians having Class I occlusion and acceptable facial aesthetics. They reported that the position of the lower lip in females was significantly more protruded than it was in males. Similarly, Erbay et al. [14] concluded that the upper and lower lips were retruded according to the norms of Steiner and Ricketts. Both the upper and lower lip values were within the normal range according to Burstone’s B line.
In the present study, it has been found that upper and lower lip when evaluated according to Steiner’s S line in males was in retro position as compared to females. However comparison of Class I and Class II showed that upper and lower lip in Class I group are significantly retrusive as compared to Class II. Erbay et al. [14] reported that the lower lip was more protrusive in the females in the dentally normal group with relation to Steiner’s reference line. However, according to Steiner’s line both lips were more protrusive in females as compared to in males in both the dentally and skeletally normal groups.
On evaluation of upper and lower lips according to Ricketts E line, similar results were obtained i.e. upper and lower lips of males was in retro position as compared to females. Erbay et al. [14] found that in females the lips were more protrusive than in males when relationship was considered to Ricketts E line. Significant difference was found between class I and class II groups. Upper and lower lip was significantly protrusive in class II group than in class I group.
In the present study, when Burstone’s B line was taken into consideration more retro positioning of upper and lower lips was seen in males than in females, but this difference was not statistically significant. However both upper and lower lips were significantly retro positioned in class I malocclusion than in class II malocclusion.
On evaluation of upper and lower lips, in relation to Sushner’s S2 line, no statistically significant differences between males and females were seen. However significant difference was seen when the comparison was made between class I and class II malocclusion. Both upper and lower lips were significantly retro positioned in class I malocclusion than in class II malocclusion. Erbay et al in 2002 compared horizontal lip position of Anatolian Turkish adults according to Sushner’s S2 line to the normal value and concluded that upper lip was more protrusive and the lower lip more retrusive compared with the normal values of Sushner. Retrusive positioning of upper and lower lip in class I malocclusion can be explained by the fact that position of lips depends upon underlying hard tissues. In class I malocclusion maxilla is normal but in class II malocclusion maxilla is protrusive or mandible is retrusive. So in class II malocclusion lips are forwardly placed as compared to those in class I malocclusion.
In the present study, on evaluating Holdaway’s H line showed no statistically significant differences on comparison between males and females. Conversely, Basciftci et al. [15] in 2004 found significant racial differences in H angle. However, on comparison between class I and class II malocclusion it was found that Holdaway’s Harmony angle in class I malocclusion is significantly less than in class II malocclusion.
Merrifield [16] in 1966 said that the Z-angle measurement and profile line provides an accurate description of the lower face relationship. A patient whose FMA, FMIA, IMPA and ANB measurements are in normal range usually has Z-angle of 80° as an adult and 78° as a child between 11 to 15 years of age. In the present study, Merrifield Z angle was found to be higher in males than in females but the difference was not significant between Class II male and Class II female group. However on comparison between skeletal Class I and Class II groups it was found that, Merrifield Z angle was significantly increased in Class I group than in class II group. Many other studies have been done on patients with different ethnic backgrounds and cultures (Nigerian, Chinese, and Japanese) [17-19]. These studies show different values for each set of population with large variability. Studies have also been done using photography and photometry to clearly evaluate the soft tissue profile or changes [20-22]. All these studies have helped in clearing the dilemma which has been present since a long time as how to achieve ideal soft tissue facial balance.
CONCLUSION
• Upper and lower lips of males were retro-positioned as compared to females and Class I group were significantly retrusive as compared to Class II according to Steiner’s S line, Rickett’s E line and Burstone’s B line
• Both upper and lower lips were significantly retro-positioned in Class I malocclusion than in Class II malocclusion according to Sushner’s S2 line.
• Holdaway Harmony angle in Class I malocclusion is significantly less than in Class II malocclusion.
• Merrifield Z angle was higher in Class I males than in Class I females. It was significantly increased in Class I group than in Class II group.
REFERENCES
- Hwang HS, Kim WS, McNamara JA Jr. A Comparative Study of Two Methods of Quantifying the Soft Tissue Profile. Angle Orthod. 2000; 70: 200-207. Ref.: https://goo.gl/y88lk3
- Subtelny JD. A longitudinal study of soft tissue facial structures and their profile characteristics, defined in relation to underlying skeletal structures. Am J Orthod. 1959; 45: 481-507. Ref.: https://goo.gl/FFsLJA
- Steiner CC. The use of cephalometrics as an aid to planning and assessing orthodontic treatment. Am J Orthod. 1960; 46: 721-735. Ref.: https://goo.gl/RRYxXM
- Ricketts RM. Esthetics, environment, and the law of lip relation. Am J Orthod. 1968; 54: 272-289. Ref.: https://goo.gl/8CalpE
- Burstone CJ. Integumental contour and extension patterns. Angle Orthod. 1959; 29: 93-104. Ref.: https://goo.gl/wGBb2X
- Holdaway RA. A soft tissue cephalometric analysis and its use in orthodontic treatment planning. Part I. Am J Orthod. 1983; 84: 1-28. Ref.: https://goo.gl/BuO2uF
- Sushner NI. A photographic study of the soft-tissue profile of the Negro population. Am J Orthod. 1977; 72: 373-385. Ref.: https://goo.gl/pSOzou
- Bowker WD, Meredith HV. A metric analysis of the facial profile. Angle Orthod. 1959; 29: 149-160. Ref.: https://goo.gl/wQoXYn
- Gulsen A, Okay C, Aslan BI, Uner O, Yavuzer R. The relationship between craniofacial structures and the nose in Anatolian Turkish adults: A cephalometric evaluation. Am J Orthod Dentofacial Orthop. 2006; 130: e15-e25. Ref.: https://goo.gl/F2T0NL
- Hwang HS, Kim WS, McNamara JA Jr. Ethnic Differences in the Soft Tissue Profile of Korean and European-American Adults with Normal Occlusions and Well-Balanced Faces. Angle Orthod. 2002; 72: 72-80. Ref.: https://goo.gl/8vlRPy
- Miyajima K, McNamara JA Jr, Kimura T, Murata S, Iizuka T. Craniofacial structure of Japanese and European-American adults with normal occlusions and well-balanced faces. Am J Orthod Dentofacial Orthop. 1996; 110: 431-438. Ref.: https://goo.gl/41WZWU
- Altemus LA. Comparative integumental relationships. Angle Orthod. 1963; 33: 217-221. Ref.: https://goo.gl/4yKqT4
- Mcnamara JA, Brust EW, Riolo ML. Soft tissue evaluation of individuals with an ideal occlusion and well balanced face. In Mcnamara JA Jr, editor. Esthetics and the treatment of facial form. Craniofacial growth series. Ann Arbor, Mich: center for human growth and development, The University of Michigan; 1992; 115-146.
- Erbay EF, Caniklioğlu CM, Erbay SK. Soft tissue profile in Anatolian Turkish adults: Part I. Evaluation of horizontal lip position using different soft tissue analyses. Am J Orthod Dentofacial Orthop. 2002; 121: 57-64. Ref.: https://goo.gl/p5mBeo
- Basciftci FA, Uysal T, Buyukerkmen A. Craniofacial structure of Anatolian Turkish adults with normal occlusions and well-balanced faces. Am J Orthod Dentofacial Orthop. 2004; 125: 366-372. Ref.: https://goo.gl/fgm2wF
- Merrifield LL. The profile line as an aid in critically evaluating facial esthetics. Am J Orthod. 1966; 52: 804-822. Ref.: https://goo.gl/rQFUpk
- Naidoo LC, Miles LP. An evaluation of the mean cephalometric values for orthognathic surgery for black South African adults. Part II: soft tissue. J Dent Assoc S Afr. 1997; 52: 545-550. Ref.: https://goo.gl/Lt24t4
- Lew KK, Ho KK, Keng SB, Ho KH. Soft-tissue cephalometric norms in Chinese adults with esthetic facial profiles. J Oral Maxillofac Surg. 1992; 50: 1184-1189. Ref.: https://goo.gl/O73723
- Alcalde RE, Jinno T, Orsini MG, Sasaki A, Sugiyama RM. Matsumura T. Soft tissue cephalometric norms in Japanese adults. Am J Orthod Dentofacial Orthop. 2000; 118: 84-89. Ref.: https://goo.gl/DSrcRT
- Scheideman GB, Bell WH, Legan HL, Finn RA, Reisch JS. Ceph- alometric analysis of dentofacial normals. Am J Orthod. 1980; 78: 404-420. Ref.: https://goo.gl/OXja61
- Yuen SWH, Hiranaka DK. A photographic study of the facial profile of southern Chinese adolescents. Quintessence International. 1989; 20: 665-676. Ref.: https://goo.gl/X6otoq
- Fernández-Riveiro P, Smyth-Chamosa E, Suárez-Quintanilla D, Suárez-Cunqueiro M. Angular Photogrammetric analysis of the soft tissue facial profile. Eur J Orthod. 2003; 25: 393-399. Ref.: https://goo.gl/zy5tU3