Case Report
Orthodontics Miniscrews to Correct an Anchorage Loss: Case Report

Houb-Dine A1* and Zaoui F2
1DDS, PhD student, Faculty of medicine and pharmacy, Mohammed V University, Rabat, Morocco
2Chief of Orthodontics Department, Faculty of Dental Medicine, Mohammed V University Rabat, Morocco
*Address for Correspondence: HOUB-DINE A, DDS, PhD student, Faculty of medicine and pharmacy, Mohammed V University, Rabat, Morocco, Email: [email protected]
Dates: Submitted: 07 February 2017; Approved: 05 April 2017; Published: 07 April 2017
How to cite this article: Houb-Dine A, Zaoui F. Orthodontics Miniscrews to Correct an Anchorage Loss: Case Report. J Oral Health Craniofac Sci. 2017; 2: 038-042. DOI: 10.29328/journal.johcs.1001009
Copyright License: 2017 Houb-Dine A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Upper molar distalization; Anchorage; Miniscrew; Temporary anchorage devices
ABSTRACT
The recent introduction of the miniscrew in orthodontics revolutionized the clinical and biomechanical approach of anchoring. Used as direct or indirect anchoring, the orthodontic micro screws indications field is expanding due to their easy insertion, and their immediate loading ensuring an absolute anchoring. Our objective through this clinical case is to show the effectiveness of these miniscrews in the correction of the uncontrolled loss of anchoring.
INTRODUCTION
Anchorage control is one of the most important keys for achievement of success in clinical orthodontics. Anchorage loss is defined as the unplanned and unexpected movement of the anchor teeth during orthodontic treatment [1]. The mesial movement of the molars in the sagittal plane, but also vertical and transverse. It may be desired or uncontrolled called also therapeutic when this controlled anchorage loss can treat a class II division 1 with or without extractions by the management of anterosuperior and posteroinferior anchoring [2].
The uncontrolled loss of anchorage means a downward revision of the therapeutic objectives involving the quality of the occlusal finishing. To get the appropriate anchorage, numerous anchorage devices are proposed and used for more than a century. Extra oral anchorages such as headgears or facemasks are the most powerful tools but they have a weak point that their effectiveness depends on the patient compliance [3]. Currently, orthodontic mini-implants, also called mini-screws or temporary anchorage devices (TAD) reduce the disadvantages of the conventional anchorage by providing an absolute anchorage, they provide additional therapeutic possibilities previously unattainable, especially in the vertical direction and in the case of posterior teeth missing [4]. The following case report will elucidate the effectiveness of the skeletal anchorage in the case of anchorage loss.
CLINICAL CASE
Adolescent female, aged 16 years with a skeletal class II hyper divergent. She had a cleft lip, 14, 24, 35 and 44 were extracted as part of an interceptive treatment by extractions at the age of 12 years but not followed by orthodontic treatment because of noncooperation. The spaces are lost by protraction of the posterior teeth with persistence of dental class II and crowding (Figures 1-3).
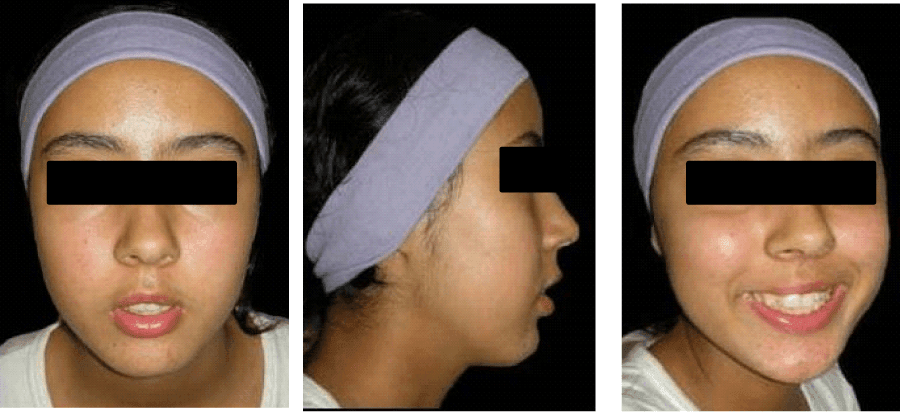
Figure 1: Pretreatment extraoral photographs of a 16-year-old female patient.

Figure 2: Initial intraoral photographs.
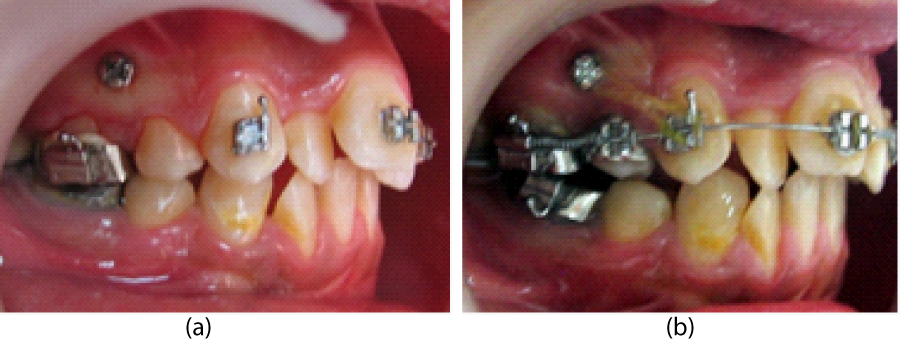
Figure 3: (a) Placement of the mini-implant between the second premolar and fi rst upper molar. (b) Distalization of the posterior teeth by indirect anchorage.
The treatment objective was the alignment of teeth and the correction of the dental class II without performing extra extractions, attenuating the bite and establishing a functional occlusion. The therapeutic approach was then oriented towards the distalization of the upper molars. In the maxilla, posterior teeth were distalized by indirect anchorage: two vestibular miniscrews (Spider Screw anchorage system with 2 mm in diameter and 8 mm long) placed into the alveolar bone (Figure 3a) between the second premolars and first upper molars were connected via Niti coil springs to the canine (Figure 3b), which receives the reactive forces of tooth movement. The canine were retracted with elastic chains directly from the mini-implant (Figure 4). To prevent flaring of the anterior teeth, the archwires were ligated passively until space was created by moving the posterior teeth distally. The treatment time was 15 months, and the case was finished with a well-aligned dentition (Figures 5-7).

Figure 4: Intraoral photographs of mid treatment during molar distalization.

Figure 5: Posttreatment intraoral photographs.
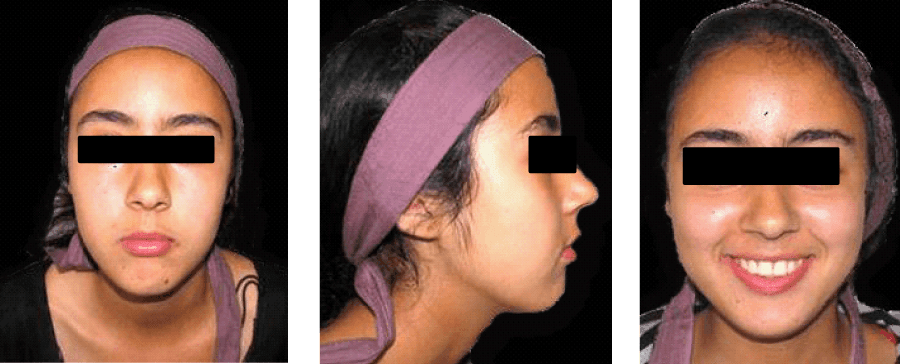
Figure 6: Posttreatment extraoral photographs.
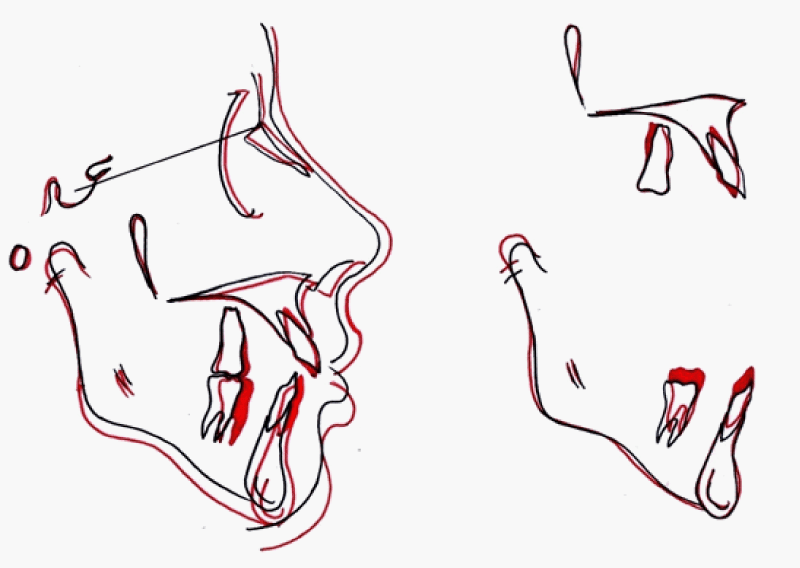
Figure 7: Superimposition of pre and post lateral cephalograms.
DISCUSSION
Mini-implants are very small screw-like gadgets used more widely in orthodontic treatments Orthodontics utilizing TAD might have advantages to treat some problems because they provide a fixed point from which to apply a force to move teeth. They can be placed in many different sites within the mouth.
In our case report, the miniscrews insertion and retrieval procedures were quick, simple, and painless. They retained their stability during treatment and were used straight away without consolidation period. There was no inflammation, bleeding, or excessive pain in the tissues adjacent to the screws and the results obtained are:
• Space gaining through distalization of upper molars by indirect anchorage
• Achievement of bilaterally Class I molar and canine relation without anterior proclination
• Comfort of the patient providing an alternative to wearing headgear without patient compliance.
• No vertical changes during upper molars distalization.
• Shorter treatment time.
Chandrakant Bangar et al. [5] think that Miniscrews and Distal Jet may be a solution. After the Distal Jet appliance has been placed and activated, palatal miniscrews are inserted between the roots of the first and second premolars, mesial to the activation locks attached to the anterior rests. The miniscrews block mesial movement of the appliance during distalization, thus preventing loss of anterior anchorage.
Antonarakis and Kiliaridis [6] found in their systematic review that tooth-borne distalizers could move maxillary molars distally on average 2.9 mm, however, the associated undesirable incisor mesial movement was 1.8 mm.
In our case, after distalization of the posterior teeth and creation of space to resolve anterior crowding and overjet, the alignment of the anterior teeth became a simple procedure without discernable forward movement of the anterior teeth and without possible deleterious effect on the facial profile. In the studies with comparable distalization techniques, the distal movements of the maxillary molars were from 3.9 to 6.4 mm [7,8], at the same time, the maxillary incisors remained stable. According to Lee JS. [9], when an orthodontic implant is used as anchorage, a space of 5 mm can be obtained by distalization of the posterior teeth predictably regardless of the cooperation of the patient.
The third molar extraction is required before distalization. Although the third molar may not always be a limitation but it may restrict the space available for the distalization of other molars, possibly posing a critical obstacle regardless of the developmental stage. Moreover, distalization increases the possibility of third molar impaction and makes the extraction of the third molar more difficult [10,11].
CONCLUSION
Orthodontic Mini implants offers many advantages when used as temporary anchorage devices like, easy placement and removal, immediate loading, can be used in a variety of locations, provide absolute anchorage, economic and requires less patient cooperation. This makes them as a necessary treatment option in cases with critical anchorage that would have otherwise resulted in anchorage loss if treated with conventional means of anchorage.
The upper molars distalization obtained in our case report of anchorage loss was a good technique. However, clinical research is recommended to establish more specific clinical guidelines.
REFERENCES
- Roberts-Harry D, Sandy J. Orthodontics. Part 9: Anchorage control and distal movement. Br Dent J. 2004 ; 196: 255-263. Ref.: https://goo.gl/pu4Q5R
- Langlade M. Thérapeutique orthodontique. 2ème édition. Maloine sa éditeur Paris. 1978; 38-48.
- Kuroda S, Tanaka E. Risks and complications of miniscrew anchorage in clinical orthodontics. Japanese Dental Science Review. 2014; 50: 79-85. Ref.: https://goo.gl/DalTth
- Lee JS, Kim JK, Park YC, Robert L, Vanarsdall Jr. Applications of orthodontic mini-implants. Quintessence International. 2007; 112-113.
- Bangar Ch, Sunil Kumar B. Temporary Anchorage Devices: A Systematic Review. Journal of Interdisciplinary Dental Sciences. 2013; 2: 19-21. Ref.: https://goo.gl/j7YSsj
- Antonarakis GS, Kiliaridis S. Maxillary molar distalization with noncompliance intramaxillary appliances in class II malocclusion. A systematic review. Angle Orthod. 2008; 78: 1133-1140. Ref.: https://goo.gl/85zHJJ
- Gelgor IE, Karaman Al, Buyukyilmaz T. Comparaison of 2 distalization systems supported by intraosseous screws. Am J Orthod Dentofacial Orthop. 2007; 131: e1-8. Ref.: https://goo.gl/w8sQjI
- Polat-Ozsoy O, Kircelli BH, Arman-Ozcirpici A, Pektas ZO, Uckan S. Pendulum appliances with 2 anchorage design: conventional anchorage vs bone anchorage. Am J Orthod Dentofacial Orthop. 2008; 133: e9-17. Ref.: https://goo.gl/F2Lhnj
- Lee JS. Development of orthodontic mini implant anchorage system. Pre-Conference: Basic Researches on Implant Orthodontics. The 4th Asian Implant Orthodontics Conference, Seoul, Korea. 2005; 3-4.
- Kim TW, Artun J, Behbehani F, Artese F. Prevalence of third molar impaction in orthodontic patients treated nonextraction and with extraction of four premolars. Am J Orthod Dentofacial Orthop. 2003; 123: 138-145. Ref.: https://goo.gl/nsTh5w
- Kandasamy S, Woods MG. Is orthodontic treatment without premolar extractions always non-extraction treatment? Aust Dent J. 2005; 50: 146-151. Ref.: https://goo.gl/QQU2Bi