Case Report
Esthetic recovery of permanent Mandibular Lateral Incisor using biological post after non-surgical healing of Periradicular Lesion: A Case Report

Amit Kumar Garg1, Neha Agrawal2* and Rajendra Kumar Tewari3 and Surendra Kumar Mishra4
1Associate Professor, Dept. of Conservative Dentistry and Endodontics, K.D. Dental College and Hospital, Mathura, India
2Associate Professor, Dept. of Periodontics and Community Dentistry, Dr. Z. A. Dental College, A.M.U., Aligarh, UP, India
3Professor and Principal, Dept. of Conservative Dentistry and Endodontics, Dr Z. A. Dental College, AMU., Aligarh,, UP, Indore, India
4Professor and Chairman, Dept. of Conservative Dentistry and Endodontics, Dr. Z. A. Dental College, A.M.U., Aligarh, UP, India
*Address for Correspondence: Dr. Neha Agrawal, MDS, Associate Professor, Dept of Periodontics and Community Dentistry, Dr. Z. A. Dental College, A.M.U., Aligarh, UP, India, Tel: 91-7895335770; Email: [email protected]
Dates: Submitted: 25 May 2017; Approved: 20 June 2017; Published: 22 June 2017
How to cite this article: Garg AK, Agrawal N, Tewari RK, Mishra SK. Esthetic recovery of permanent Mandibular Lateral Incisor using biological post after non-surgical healing of Periradicular Lesion: A Case Report. J Oral Health Craniofac Sci. 2017; 2: 064-068. DOI:10.29328/journal.johcs.1001013
Copyright License: 2017 Garg AK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: Biological post; Calcium hydroxide; Triple antibiotic paste
ABSTRACT
Statement of the problem: Anterior tooth fracture, as a result of traumatic injuries, frequently occurs in dentistry. This leads to necrosis of pulp and periapical pathology. The goal of endodontic and restorative dentistry is to retain natural teeth with maximum function and pleasing esthetics.
Purpose of the study: This study aimed at proper reconstruction of extensively damaged teeth through the procedure known as “Biological Restoration.”
Materials and methods: Biological post obtained through natural, extracted teeth from another individual represents a low-cost option and alternative technique for the morphofunctional recovery of damaged anterior teeth that provides highly functional and esthetic outcomes.
Conclusions: This case report refers to the esthetics and functional recovery of mandibular left lateral incisor after non-surgical healing of periradicular lesion.
INTRODUCTION
The manifestations of trauma can vary from simple enamel-dentin fracture to complicated crown-root fracture [1]. The patient commonly reports after many years when necrosis of the pulp has caused apical periodontitis or discoloration, causing either pain or compromised esthetic. Inadvertently, radiographs reveal periapical pathology. The most important objective of endodontic treatment of teeth with necrotic pulp and periapical lesions is the elimination of infection from the root canal system [2]. Disinfection is achieved by irrigation followed by the placement of an intracanal medicament. The goal of endodontic and restorative dentistry is to retain natural teeth with maximum function and pleasing esthetics. Recently, Extracted tooth fragments can also be used to make a dent in post for reinforcing the root canal in grossly decayed teeth. Dentin posts have been used in the primary dentition with promising clinical and laboratory results [3,4]. The purpose of the present article is to describe a multidisplinary approach to restore a mandibular lateral incisor using biological post after non-surgical endodontic treatment in permanent dentition. Till date, this is the only case report of using biological post in permanent dentition.
CASE REPORT
The tooth is MANDIBULAR LEFT LATERAL INCISOR (#23). The patient gave a history of trauma to her anterior teeth when she was 22 years old. The patient’s medical history was unremarkable. History of dental treatment was present for same tooth. Intraoral examination revealed discolored and fractured tooth #23 with sinus tract. Tooth failed to respond to thermal and electric pulp testing. The tooth had grade 2 mobility and periodontal pocket. A periapical radiograph revealed a radiolucent lesion involving the apex of tooth #23 (Figure 1A). After extensive clinical and radio graphical examination, the diagnosis of chronic periapical periodontitis with necrotic pulp was made. Esthetic restoration with intraradicular reinforcement by means of a dentin post was planned for tooth #23. This study was approved by institutional ethical review board. The patient was informed about the proposed treatment and signed a written consent form authorizing the completion of the procedure, as the dentin post is made from extracted teeth.
Local anesthesia was induced with 2% lidocaine containing 1:80,000 epinephrine. A rubber dam was applied and coronal access was made. The root canal was explored with a K-file #15. The radio graphical length measurement was performed (Figure 1B) and confirmed with an electronic apex locator. The root canal was shaped with hand K-file to a size 30K-file. During preparation, EDTA was used as lubricant and the root canal was disinfected with 2.5 % sodium hypochlorite solution.
The intracanal dressing of calcium hydroxide was given for one month (Figure1C). At the one month recall, the patient was asymptomatic, with no signs of the sinus tract. Then, intracanal dressings of triple antibiotic paste (ciprofloxacin/ metronidazole/ minocycline) (Figure 1D) were given for next 5 months, as described by Hoshino et al. At the 6-months follow-up, the patient was still asymptomatic, and the radiolucent area was absent on periapical radiograph. Conventional endodontic treatment was performed using AH-plus sealer and gutta-percha (Figure 1E). The obturating material of the root was removed using peeso-reamer and 5mm of gutta-percha was left in apical third, and the root was prepared to receive intracanal portion of the biological post (Figure 1F,G).
These dentin posts were obtained from extracted teeth (Figure 1H) and underwent sterilization. The shaped dentin post was then tried for fit in the prepared root canal and readjusted for a snug fit. The root canal space and dentin post were etched with 35% orthophosphoric acid (Etchant Gel S, Coltene Whaledent, Switzerland) for 15 seconds. The root canal space and dentin post were rinsed thoroughly with water until all traces of etchant had been removed and dried with pressurised oil-free air. The bonding agent (One Coat Bond, Coltene Whaledent) was applied in root canal space and on dentin post with the help of brush and massaged it for 20 seconds and air dried gently, then lightcured for 10 seconds (LED-polymerisation devices with light power levels >800mW/cm2. The ParaCem cement (“ParaCem Universal, Coltene whaledent, Switzerland”) WAS placed in the root canal; the post is placed in position. The excess cement WAS removed, and light-polymerization WAS done with LED curing light (Figure 1I). To reconstruct the crown preparation the same ParaCem cement WAS used. The rough margin present labially as well as palatally made smooth and extra cement removed using composite polishing kit Soϐlex (Shofu, Japan). The crown WAS prepared to obtain the desired aesthetic effect (Figure 1J).
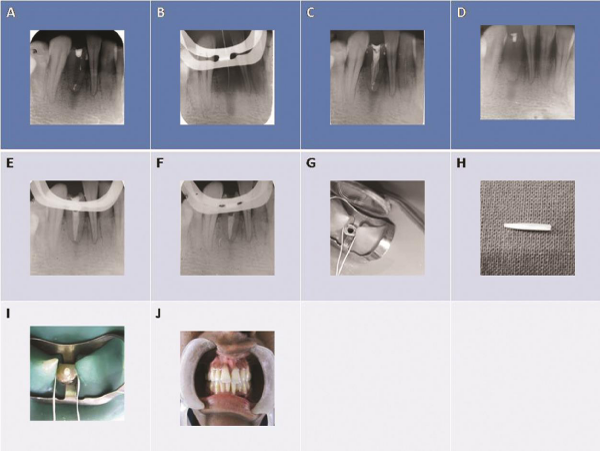
Figure 1: Preoperative radiograph of mandibular left lateral incisor (#23). A. Working length radiograph of tooth (#23). B. Radiograph of tooth (#23) with intracanal dressing of calcium hydroxide. C. Radiograph of tooth (#23) with intracanal dressing of triple antibiotic paste. D. Radiograph showing obturation of tooth (#23). F, G. Tooth (#23) was prepared to receive intracanal portion of the biological post. H. Dentin post was obtained from extracted teeth. I. Biological post was cemented in the tooth (#23). J. Final aspect of the tooth after esthetic recovery of tooth (#23).
DISCUSSION
It is evident that an infected root canal system is a unique niche for the selective species of microorganisms. Microflora of teeth with persistence disease showed a high prevalence of enterococci and streptococci followed by lactobacilli, Actinomyces species, peptostreptococci, Candida, Eubacterium alactolyticus, Propionibacterium propionicum, Dialister pneumosintes and Filifactor alocis [5]. Links between endodontic inflammation and cardiovascular outcomes are biologically plausible, considering the predominance of Gram-negative anaerobes associated with endodontic infections [6,7], evidence of cytokine production in inflamed pulp and periapical granulomatous tissues [8], and observations of elevated systemic levels of inflammatory mediators in endodontic patients [9,10].
A common protocol for management of infected mature teeth with apical periodontitis is to place calcium hydroxide in the root canal system for 1 to 4 weeks. Calcium hydroxide is the most commonly used endodontic intracanal dressing materials because of its high pH and favorable effects such as antibacterial and hard tissue stimulation [11]. Its broad spectrum antibacterial activity is another major factor for its wide spread use and therapeutic success. The studies have shown that root canal filling with calcium hydroxide reduced the strength of dentin of mature human teeth [12]. To prevent this detrimental effect, another intracanal medicament has been developed. In recent years, The Cardiology Research Unit of the Niigata University has developed the concept of ‘Lesion sterilization and tissue repair LSTR’ therapy [13], that employs the use of a combination of antibacterial drugs (triple antibiotic paste) for disinfection pulpal and periradicular lesions. Triple antibiotic paste consists of ciprofloxacin, metronidazole and minocycline [14]. In some case reports, triple antibiotic paste was also reported to provide successful management of a periapical lesion with sinus tract [15]. It causes effective destruction of all kinds of endodontic pathogens aerobic as well as anaerobic. A disadvantage of this mixture is tooth discoloration to a bluish-grey hue. The discoloration brought about by tetracycline family is believed to be due to photo-induced reaction. Minocycline binds to calcium-ions through chelation reaction; forming an insoluble molecule [16]. Repair of damaged tissues can be expected if lesions are disinfected [17]. In the present study, tooth #23 was healed non-surgically using combination of calcium hydroxide and triple antibiotic paste.
The restorative treatment of fractured teeth directly affects the treatment prognosis and requires a careful consideration of several factors, such as extent and pattern of the fracture, and the additional form of retention and stability, which is commonly achieved by the use of screw-posts, cast posts, or dentin pins [18]. Steel and titanium posts have an increased risk of tooth fracture when subjected to occlusal loads [19]. When a fiber post is subjected to same loads, debonding of post- restoration joint occurs. The use of biological post provides an esthetic, biocompatible, and low cost material, as biological posts are made from donated extracted natural teeth [4,20]. The physical properties are similar to the original tooth and shows excellent adhesion to the remaining tooth structure and composite resin. In this case, biological post was used for esthetic recovery of tooth #23. Concerning the ethical aspect, it is necessary to clarify to the patient and or her parents or guardian that the post is made from duly donated and properly autoclaved extracted teeth, thus preventing biosecurity risks. However, patient acceptance of a biological restoration is an important issue and donor selection from siblings could be a more acceptable alternative.
CONCLUSION
This case report refers to the proper reconstruction of esthetics and functions of mandibular left lateral incisor after non-surgical healing of periradicular lesion using biological restoration.
REFERENCES
- Holan G, Shmueli Y. Knowledge of physicians in hospital emergency rooms in Israel on their role in cases of avulsion of permanent incisors. Int J Paediatr Dent. 2003; 13: 13-19. Ref.: https://goo.gl/EdNWMm
- Elkarim I, Kennedy J, Hussey D. The antimicrobial effects of root canal irrigation and medication. Oral Surg Oral Med Oral Pathol. 2007; 103: 560-569. Ref.: https://goo.gl/sTmTyk
- Pinheiro SL, Bonecker MJ, Duarte DA, Imparato JC, Oda M. Bond strength analysis of intracanal posts used in anterior primary teeth: An in vitro study. J Clin Pediatr Dent. 2006; 31: 32-34. Ref.: https://goo.gl/wxtx3r
- Kaizer OB, Bonfante G, Pereira Filho LD, Cardinal L, Reis KR. Utilization of biological posts to reconstruct weakened roots. Rev Gaucha Odontol. 2008; 56: 7-13.
- Siqueira JF Jr, Rocas IN. Polymerase chain reaction- based analysis of microorganisms associated with failed endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2004; 97: 85-94. Ref.: https://goo.gl/vyt8Kw
- Baumgartner JC. Microbiologic and pathologic aspects of endodontics. Curr Opin Dent. 1991; 1: 737-743. Ref.: https://goo.gl/Sgjuoo
- Sundqvist G. Ecology of the root canal flora. J Endod. 1992; 18: 427-430. Ref.: https://goo.gl/pPYBMB
- Barkhordar RA, Hayashi C, Hussain MZ. Detection of interleukin-6 in human dental pulp and periapical lesions. Endod Dent Traumatol. 1999; 15: 26-27. Ref.: https://goo.gl/z7HTft
- Marton I, Kiss C, Balla G, Szabo T, Karmazsin L. Acute phase proteins in patients with chronic periapical granuloma before and after surgical treatment. Oral Microbiol Immunol. 1988; 3: 95-96. Ref.: https://goo.gl/8esh5p
- Marton IJ, Kiss C. Influence of surgical treatment of periapical lesions on serum and blood levels of inflammatory mediators. Int Endod J. 1992; 25: 229-233. Ref.: https://goo.gl/2AekA1
- Zmener O, Pameijer CH, Banegas G. An in vitro study of the pH of three calcium hydroxide dressing materials. Dent Traumatol. 2007; 23: 21-25. Ref.: https://goo.gl/pKU7Qe
- Sahebi S, Moazami F, Abbott P. The effect of short-term calcium hydroxide application on the strength of dentine. Dent Traumatol. 2010; 26: 43-46. Ref.: https://goo.gl/WHN5Bn
- Hoshino E, Takushige T. LSTR 3Mix-MP method-better and efficient clinical procedures of lesion sterilization and tissue repair (LSTR) therapy. Dent Rev. 1998; 666: 57-106.
- Sato I, Ando‐Kurihara N, Kota K, Iwaku M, Hoshino E. Sterilization of infected root‐canal dentine by topical application of a mixture of ciprofloxacin, metronidazole and minocycline in situ. Int Endod J. 1996; 29: 118-124. Ref.: https://goo.gl/bLvftS
- Siqueira JF, Rôças IN, Alves FR, Silva MG. Bacteria in the apical root canal of teeth with primary apical periodontitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107: 721-726. Ref.: https://goo.gl/e9THjf
- Kim JH, Kim Y, Shin SJ, Park JW, Jung IY. Tooth discoloration of immature permanent incisor associated with triple antibiotic therapy: A case report. J Endod. 2010; 36: 1086-1091. Ref.: https://goo.gl/twbxXS
- Takushige T, Cruz EV, Asgor Moral A, Hoshino E. Endodontic treatment of primary teeth using a combination of antibacterial drugs. Int Endod J. 2004; 37: 132-138. Ref.: https://goo.gl/BAqTTW
- Oz IA, Haytac MC, Toroglu MS. Multidisciplinary approach to the rehabilitation of a crown-root fracture with original fragment for immediate esthetics: A case report with 4-year follow-up. Dent Traumatol. 2006; 22: 48-52. Ref.: https://goo.gl/pKuuB1
- Isidor F, Odman P, Brondum K. Intermittent loading of teeth restored using prefabricated carbon fiber post. Int J Prosthodont. 1996; 9: 131-136. Ref.: https://goo.gl/8mvG6A
- Corrẻa-Faria P, Alcảntara CEP, Caldas-Diniz MV, Botelho AM, Tavano KTA. Biological restoration: root canal and coronal reconstruction. J Esthet Restor Dent. 2010; 22: 168-178. Ref.: https://goo.gl/GM7Xhg