
More Information
Submitted: July 25, 2023 | Approved: August 07, 2023 | Published: August 08, 2023
How to cite this article: Alanazi M, Alanazi W, Alali H, Alnoaimi F, Shuwaykan A, et al. Knowledge, Attitude, and Practices of Parents toward (Infant & Child) Oral Health in Family Medicine Center at PSMMC, Riyadh. J Oral Health Craniofac Sci. 2023; 8: 016-023.
DOI: 10.29328/journal.johcs.1001044
Copyright License: © 2023 Alanazi M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Keywords: BoneAttitude; Knowledge; Oral health; Parents; Practice

Knowledge, Attitude, and Practices of Parents toward (Infant & Child) Oral Health in Family Medicine Center at PSMMC, Riyadh
Maryam Alanazi1, Wed Alanazi2, Hanan Alali3, Fatma Alnoaimi3, Arwa Shuwaykan4 and Nuha Al-Yahya5
1Senior Dental Hygienist, Department of Oral and Dental Health Specialist, Dental Center, PSMMC, Riyadh, Saudi Arabia
2Department of General Density, Dental Center, PSMMC, Riyadh, Saudi Arabia
3Dental Hygienist, Department of Oral and Dental Health Specialist, Dental Center, Riyadh, Saudi Arabia
4Dental Assistant, Dental Center, PSMMC, Riyadh, Saudi Arabia
5Laboratory Specialist, Statistical, PSMMC, Riyadh, Saudi Arabia
*Address for Correspondence: Maryam Alanazi, Senior Dental Hygienist, Department of Oral and Dental Health Specialist, Dental Center, PSMMC, Riyadh, Saudi Arabia, Email: [email protected]
Background: Early childhood caries may develop as soon as teeth erupt. Promoting oral health care programs is very important and helps to reduce dental caries in young children. The aim of this study was to assess the infant/child oral health (IOH) related knowledge, attitudes, and practices (KAP) of parents in Riyadh, Saudi Arabia.
Materials and Methods: A cross-sectional descriptive study was conducted among 327 parents. Visiting the family medicine center at prince sultan military medical city, Riyadh Saudi Arabia. A 39-item questionnaire covering socio-demographic characteristics and questions pertaining to KAP regarding OH care will be used to collect the data. Descriptive statistics, Student’s t-test, one-way analysis of variance, and Scheffe’s test will use for the statistical analysis (p ≤ 0.05).
Results: The result showed that the majority of the parents had good knowledge regarding OH, knowledge of cleaning (92.4.%), and knowledge of the amount of sugar (88.1.%). the parent’s age group (30 to 39) years (n =147) reported the highest mean (knowledge, attitudes, and practice) scores among all other age groups with a knowledge mean score of (6.80 ± 1.73), an attitude mean score of (8.86 ± 1.37), and a practice mean score of (5.14 ± 1.86). Female parents showed significantly higher mean knowledge, attitude, and practice scores than male parents. In addition, the middle-income level parents’ group (n = 295) reported higher knowledge mean score compared to the low-income parents’ group (n = 15) with a mean difference of d = 1.15, p = .041.
Conclusion: Parents’ knowledge about maintaining oral and dental health care for infants/children was inadequate. Essentially, medical professionals are the initial ones to interact with expecting and new moms. Therefore, need to raise parents’ awareness about oral and dental health for infants/children, through the development and implementation of long-term education and promotions programs.
Infant Oral Health (IOH) is the foundation upon, which preventive education and dental care must be built to enhance the opportunity for lifetime freedom from preventable oral diseases [1]. Parents are the decision-makers in matters of health care for children; thus, they play an important role in achieving the best oral health outcomes for their young children [2]. It is therefore expected that the preventive oral health behavior of parents for children would influence their children’s behavior in adapting preventive oral health practices as they grow along [3]. Early Childhood Caries (ECC) is an infectious and preventable disease that is transmitted vertically from mothers or other intimate caregivers to infants.
Modification of the mother’s oral hygiene, diet, and the use of topical fluorides can have a significant impact on the child’s caries rate [1]. Since parents/guardians are responsible for almost all health issues related to their children, their role in modeling their children toward practicing preventive oral health throughout life is crucial [4]. Thus, parents/guardians should be educated about oral health care for their children from inception through the existing setup. Studies eliciting parental knowledge, attitudes, and preventive behaviors on the oral health of children are scanty [4-6]. Considering, parent’s important role in the well-being of young children, it is essential to explore their Knowledge, Attitude, and Practices (KAP) as it affects the dental care that children receive at home and their access to professional dental services. Furthermore, their assumptions and beliefs may be an important consideration in attempts made to improve IOH. Thus, this study was undertaken to assess the IOH-related KAP of parents having children aged 2 months to 6 years in a family medicine center, PSMMC, Riyadh, Saudi Arabia.
Study design and study setting
A descriptive study will conduct in Family Medicine Centre (vaccination clinic & dental prevention & education clinic). An online questionnaire will send it to all booked patients through (SMS) AFTER check-in. Ethical approval was obtained from the Dental Research Committee at PSMMC. A 39-item questionnaire covering socio-demographic characteristics and questions pertaining to KAP regarding OH care was used to collect the data. Descriptive statistics, Student’s t-test, one-way analysis of variance, and Scheffe’s test will use for the statistical analysis (p ≤ 0.05).
Inclusion criteria: Parents having children aged 2 months to 6 years; who are having vaccinations appointments or visiting the dental prevention clinic, who will willing to participate and also sign the informed consent.
Exclusion criteria: Parents who could not read and write.
Sampling and sample size
All the parents of children aged 2 months to 6 years, who visited the family medicine center (infant & child vaccine clinics) were informed about the purpose of the survey and were invited to participate. Those who fulfilled the above-mentioned eligibility criteria were included in the survey. Based on convenience sampling, a total sample size of 325 was obtained.
Pilot study
A pilot survey was conducted among 45 eligible parents to assess the reliability of the Questionnaire, the feasibility of conducting the survey, and the sample size calculation. Based on the 50% prevalence, 95% confidence level, and 10% precision of OH - KAP (our main outcome) among parents and the minimum sample size was estimated as 300.
Methodology
The validation questionnaire was translated into the local language (Arabic) and was validated through a pretested survey. Validity indicates whether the instrument appears to be assessing the desired qualities. It was observed that 95% of the participants found the questionnaire to be easy. The validity mean ratio was calculated as 0.87 based on the opinions expressed by a panel of academicians. The questionnaire consisted of 39 questions as follows: 1- six questions to gather information related to parents’ demographic. Characteristics include gender, age, employment, educational level, and monthly income. 2- Nine multiple choice questions to assess the IOH care knowledge among parents. 3- Twelve questions aimed to explore the attitude of parents regarding IOH care. 4- Twelve questions were aimed to investigate the practices of parents regarding IOH care.
A descriptive analysis of respondents’ demographic characteristics provided showed that 63.6% (N=208) of the respondents were mothers, 32.1% (n = 105) fathers, and 4.3% (n = 14) others. In terms of infants/Child’s relatives’ age, 6.6% (n = 22) were between 20 and 29, 45% (n = 147) were between 30 and 39, 41.9% (n = 137) were 40 to 49, and 6.5% (n = 21) were 50 and above. For the respondents’ educational level, 57.2% (n = 187) had completed a Bachelor’s degree, 22.6% (N=74) high school level, 10% (n = 33) postgraduate level, 10% (n = 33) middle school level, 4.3% (n = 14) elementary school level, and 2.8% (n = 9) other levels of education. 4.6% (n=15) of the respondents had a low income, whereas 90.2% (n = 295) had a middle income, and 5.2% (n = 17) high income. 57.8% (n = 186) reported that their child’s gender is male, while 42.2% (n = 138) answered with the female. Regarding the age of Childs, 87.5% (n = 286) stated their child was two years or more, 8.2% (n = 27) one-year-old, 3.1% (n = 10) six months old, and 1.2% (n = 4) two months old (Table 1).
| Table 1: Demographical Characteristics (n = 327). | ||
| Demographic | Frequency | Percentage |
| Respondent | ||
| Mother | 208 | 63.6 |
| Father | 105 | 32.1 |
| Other | 14 | 4.3 |
| Age | ||
| 20 - 29 | 22 | 6.6 |
| 30 - 39 | 147 | 45 |
| 40 - 49 | 137 | 41.9 |
| 50 and above | 21 | 6.5 |
| Education Level | ||
| Bachelor | 187 | 57.2 |
| High School | 74 | 22.6 |
| Post Graduate | 33 | 10 |
| Middle School | 14 | 4.3 |
| Elementary School | 10 | 3.1 |
| Other | 9 | 2.8 |
| Income Level | ||
| Low Income | 15 | 4.6 |
| Middle Income | 295 | 90.2 |
| High Income | 17 | 5.2 |
| Gender of Infant/Child | ||
| Male | 186 | 57.8 |
| Female | 138 | 42.2 |
| Age of Infant/Child | ||
| Two years and more | 286 | 87.5 |
| One year | 27 | 8.2 |
| Six Months | 10 | 3.1 |
| Two Months | 4 | 1.2 |
When looking at the respondents’ responses to knowledge questions, results show that 63.9% (n = 209) answered NO to the question; fruit juice for children is not good for teeth, while 36.1% (n = 118) answered YES. 88.1% (n = 288) answered YES to the question; Sugar is found in most food and beverages for children, while 11.9% (n = 39) said NO. 91.4% (n = 299) answered YES to the question; Fluoride is beneficial in oral health, whereas 8.6% (n = 28) said NO. 79.8% (n = 261) answered YES to the question about knowing the recommended amount of toothpaste to use, while 20.2% (n = 66) responded with NO (Figure 1).
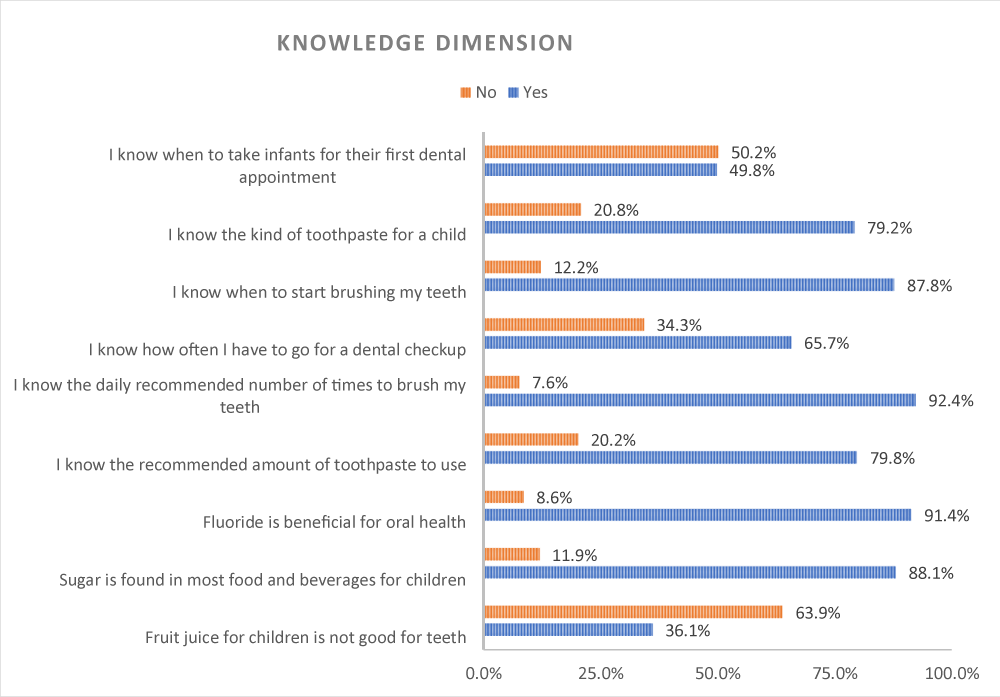
Figure 1: Distribution of Infants/Childs’ Relatives’ Responses towards Knowledge Dimension Items (n = 327).
In light of the respondents’ attitudes, 34.3% (n = 112) agree with the statement; tooth decay is caused by bacteria that are transmitted by sharing feeding utensils, while 65.7% (n = 215) disagree. 99.4% (n = 325) agree that; a balanced diet is essential for the healthy growth of the baby’s diet, whereas 0.6% (n = 2) disagree. 55% (n = 180) agree with the statement; night time bottle/breastfeeding can cause tooth decay, while 45% (n = 147) disagree. 94.2% (n = 308) agree that; a child’s teeth should be brushed/cleaned, while 5.8% (n = 19) disagree (Figure 2).
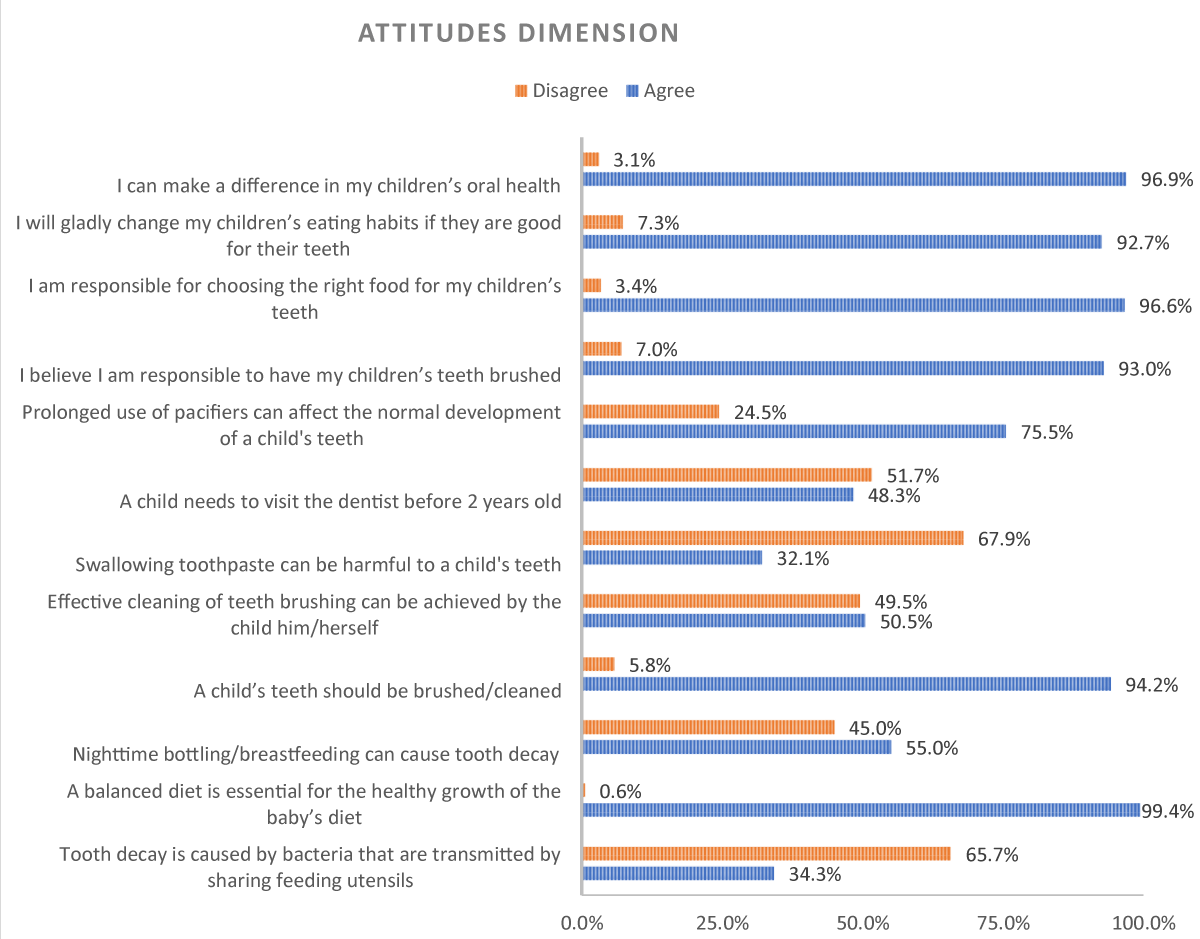
Figure 2: Distribution of Infants/Childs’ Relatives’ Responses towards Attitudes Dimension Items (n = 327).
Considering the respondents’ practices, 48.6% (n = 159) revealed they always bite the food into small pieces before giving it to the child, whereas only 2.5% (n = 8) said they never did so. 64.2% (n = 210) of the respondents said they sometimes give sweet food to the child (liquid/solid), with only 5% (n = 16) saying they never do. On the question on starting semisolid food on their children 40.7% (n = 133) said they sometimes did it in the first 6 months and 41.9% (n = 137) in the first year. 40.1% (n = 131) said they always started semisolid food on their children in one year and a half to two years, while 57.8% (n = 189) said they always carried out the practice in two years and more (Figure 3).
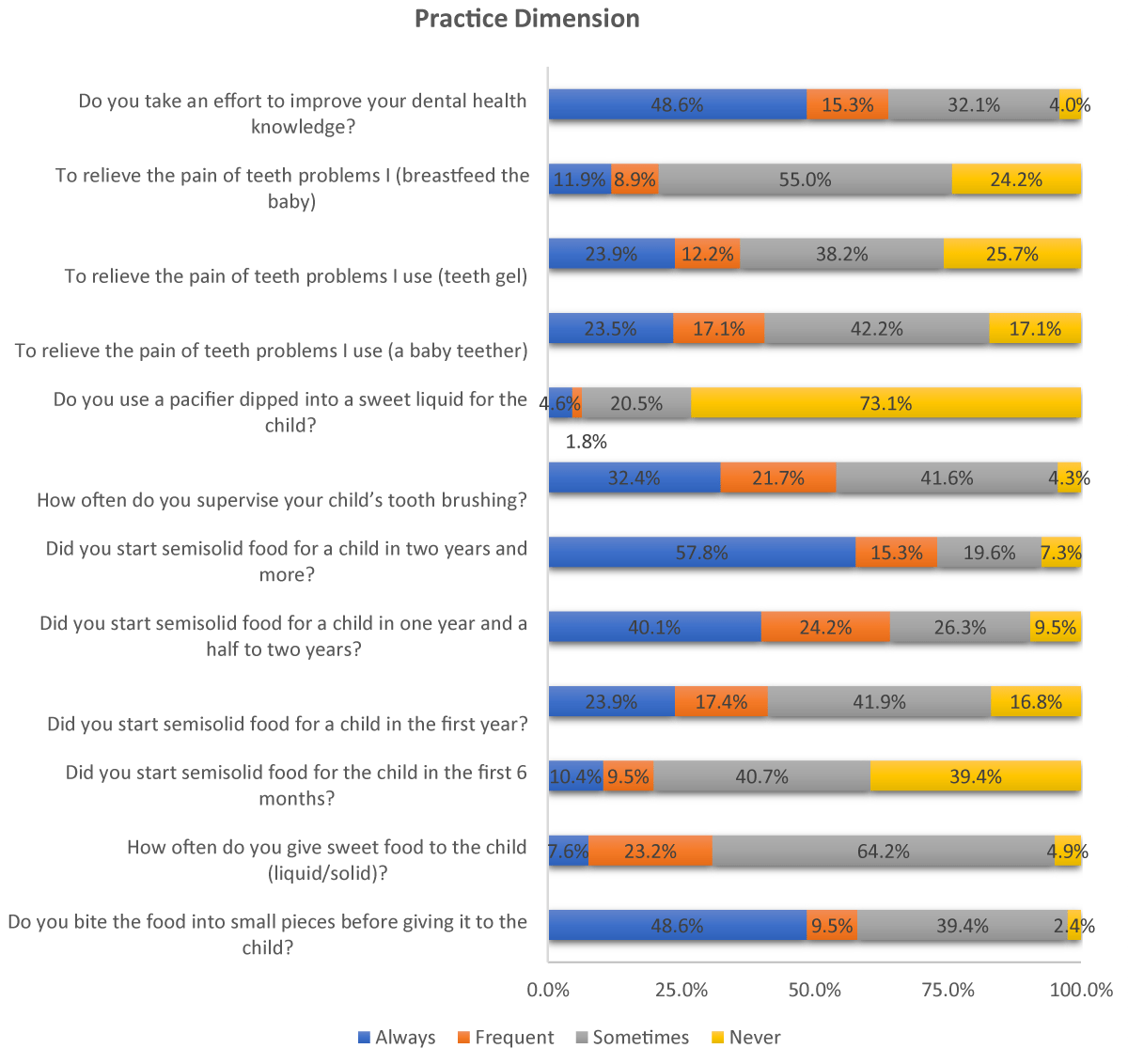
Figure 3: Distribution of Infants/Childs’ Relatives’ Responses towards Practice Dimension Items (n = 327).
Furthermore, Respondents were asked about how much toothpaste they use to brush their children’s teeth, 29.4% (n = 96) said a smear, 49.8% (n = 163) mentioned they use pea size, while 4.3% (n = 14) said they do not use toothpaste (Figure 4).
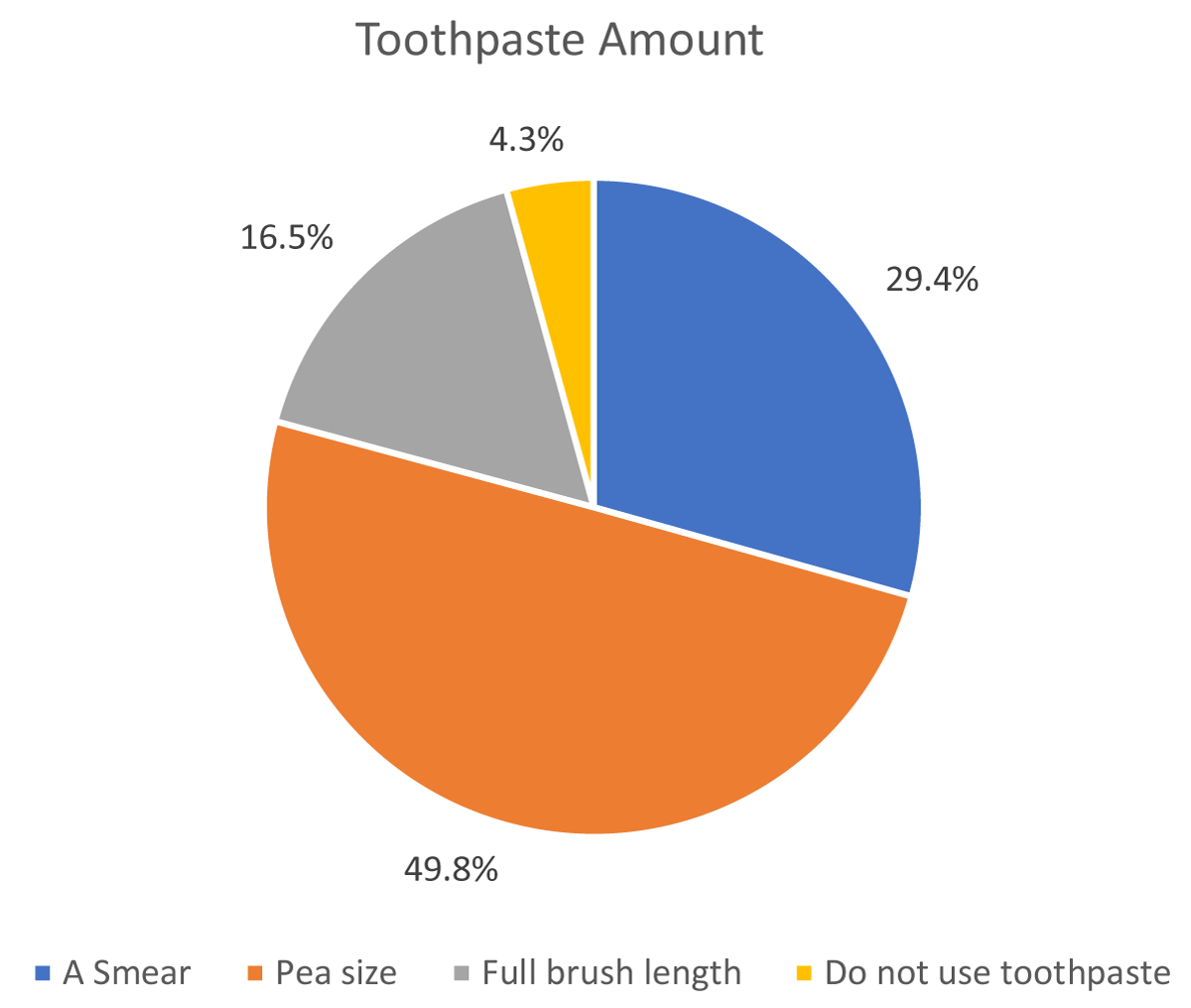
Figure 4: Distribution of Respondents according to the Amount of Toothpaste They Use for Brushing Teeth of their Infants/Childs (n = 327).
Descriptive statistics (Mean: M± Standard deviation: SD) for (knowledge, attitudes, and practice) scores among responded parents according to their age (in years) are summarized in Table 2. It is clear that parents of age group (30 to 39) years (n = 147) reported the highest mean (knowledge, attitudes, and practice) scores among all other age groups with a knowledge mean score of (6.80 ± 1.73), an attitude mean score of (8.86 ± 1.37), and a practice mean score of (5.14 ± 1.86).
| Table 2: Assessment and comparison of mean knowledge, attitude, and practices scores according to the age of the parents | ||||||
| Variables | Age in years | N Total = 327 |
Mean | Standard deviation | Standard error | P value |
| Knowledge |
20 - 29 | 22 | 6.14 | 1.67 | 0.36 | .353 |
| 30 - 39 | 147 | 6.80 | 1.73 | 0.14 | ||
| 40 - 49 | 137 | 6.72 | 1.67 | 0.14 | ||
| 50 and above | 21 | 6.48 | 2.02 | 0.44 | ||
| Attitude | 20 - 29 | 22 | 8.73 | 1.67 | 0.36 | .256 |
| 30 - 39 | 147 | 8.86 | 1.37 | 0.11 | ||
| 40 - 49 | 137 | 8.55 | 1.70 | 0.15 | ||
| 50 and above | 21 | 8.29 | 1.87 | 0.41 | ||
| Practices | 20 - 29 | 22 | 4.59 | 1.37 | 0.29 | .201 |
| 30 - 39 | 147 | 5.14 | 1.86 | 0.15 | ||
| 40 - 49 | 137 | 4.72 | 1.81 | 0.15 | ||
| 50 and above | 21 | 4.71 | 1.90 | 1.82 | ||
Analysis of variance (ANOVA) test was used to figure out if there are statistically significant differences in (knowledge, attitudes, and practice) mean scores among responded parents’ age (in years) at a significance level of 0.05. Results revealed through data analysis show that there are NO statistically significant differences in (knowledge, attitudes, and practice) mean scores referring to the responded parent’s age (in years) at the significance level of 0.05 (Table 2).
Descriptive statistics (Mean: M± Standard deviation: SD) for (knowledge, attitudes, and practice) scores among responded parents according to their income level are summarized in Table 2. It is clear that parents of the high-income group (n = 147) reported the highest mean (knowledge, and attitudes) scores among all other income groups with a knowledge mean score of (6.94 ± 1.71) and an attitude mean score of (8.66 ± 1.59). While parents of the low-income group (n = 15) reported the highest mean practice scores among all other income groups with a practice mean score of (5.20 ± 2.37).
Scheffe’s Post hoc tests show that there are statistically significant differences in knowledge mean score referring to the responded parent’s monthly income level at the significance level of 0.05. Where, the middle-income level parents’ group (n = 295) reported higher knowledge mean score compared to the low-income parents’ group (n = 15) with a mean difference of d = 1.15, p = .041. On the other hand, results show that there are NO statistically significant differences in attitudes nor practice mean scores referring to the responded parent’s monthly income level at the significance level of 0.05 (Table 3).
| Table 3: Assessment and comparison of mean knowledge, attitude, and practices scores according to the income level of the parents. | ||||||
| Variables | Monthly income level | N Total = 327 | Mean | Standard deviation | Standard error | p value |
| Knowledge | Low Income | 15 | 5.60 | 1.96 | 0.51 | .035 |
| Middle Income | 295 | 6.75 | 1.69 | 0.10 | ||
| High Income | 17 | 6.94 | 1.71 | 0.42 | ||
| Attitude | Low Income | 15 | 8.60 | 1.18 | 0.31 | .332 |
| Middle Income | 295 | 8.66 | 1.59 | 0.09 | ||
| High Income | 17 | 9.24 | 1.60 | 0.39 | ||
| Practices | Low Income | 15 | 5.20 | 2.37 | 0.61 | .777 |
| Middle Income | 295 | 4.89 | 1.78 | 0.10 | ||
| High Income | 17 | 4.76 | 2.11 | 0.51 | ||
Descriptive statistics (Mean: M± Standard deviation: SD) for (knowledge, attitudes, and practice) scores among responded parents according to their relationship with infant/Child are summarized in Table 3. It is clear that Mothers of infants/Childs (n = 208) reported the highest mean (knowledge, attitudes, and practice) scores among all other relation type groups with a knowledge mean score of (6.96 ± 1.57), an attitude mean score of (8.95 ± 1.33), and a practice mean score of (5.17 ± 1.82).
Scheffe’s Post hoc tests show that there are statistically significant differences in knowledge mean score referring to the relation type of infant/Child’s parent at the significance level of 0.05. Where, Female parents (n = 208) reported higher knowledge mean score compared to Male parents (n=105) with a mean difference of d = 0.73, p = .002. In addition, results show that there are statistically significant differences in attitude mean scores referring to the sex of the infant/Child’s parent at the significance level of .05. Where Female parents reported higher attitude mean scores compared to Male parents with a mean difference of d = 0.72, p = .001. Finally, data analysis shows that there are statistically significant differences in practice mean score referring to the sex of the infant/Child’s parent at the significance level of 0.05. Where, Female parents reported higher practice mean scores compared to Male parents with a mean difference of d = 0.79, p = .001 (Table 4).
| Table 4: Assessment and comparison of mean knowledge, attitude, and practices scores according to the relation type to infant/Child of responded parents. | ||||||
| Variables | Relative type of parents | N Total = 327 | Mean | Standard deviation | Standard error | p value |
| Knowledge | Mother | 208 | 6.96 | 1.57 | 0.11 | .001 |
| Father | 105 | 6.23 | 1.86 | 0.18 | ||
| Other | 14 | 6.43 | 2.06 | 0.55 | ||
| Attitude | Mother | 208 | 8.95 | 1.33 | 0.09 | <.001 |
| Father | 105 | 8.23 | 1.89 | 0.18 | ||
| Other | 14 | 8.14 | 1.61 | 0.43 | ||
| Practices | Mother | 208 | 5.17 | 1.82 | 0.13 | .001 |
| Father | 105 | 4.38 | 1.78 | 0.17 | ||
| Other | 14 | 4.79 | 1.31 | 0.35 | ||
Childhood oral health correlates to their parents’ or caregivers’ oral health awareness. In the words of Dagon, et al. [6], early childhood is when oral health-related routines, including those relating to diet and oral cleanliness, develop and remain consistent. Parents serve as examples for their kids, as noted by Burgette and Chi [4]. In light of relative risk variables and protective variables that get predicted to have an impact on young children’s dental wellness and the influence of socioeconomic circumstances on parent’s oral hygiene knowledge, attitude, and practices, this study provides information about caregivers and parents’ understanding, perspective, and practices concerning the dental well-being of children.
For this study, 327 parents got surveyed, where 208 of them, or 63.6% were mothers. This information is available in Table 1. The results are understandable since mothers are the parental figures who interact with kids around this age range most frequently in society. Dahlan, et al. [7] note that the American Academy of Pediatric Dentistry advises that kids should visit a dentist when they are less than twelve months of maturity and no earlier than six months after the emergence of their initial primary tooth. Hancock, Schofield, and Zinn [8] reveal that the traditional belief regarding the developmental age for a first dental visit was three years old. The opinion appeared justified because kids at that stage are easier to handle and will respond better to treatment.
Parenting styles are changing thanks to the rising number of households and the busy, aggressive work environment. Ramos-Gomez [9] suggests numerous advantages of breastmilk in an infant’s first year. However, Wahyuni, Rutina, and Efendi [10] found a link between early childhood cavities, lactation, and baby bottle use after 12 months, particularly if extensive or overnight. Ramos Gomez [9] points out that during the first six months associated with existence, infants should only get breastfed before introducing iron-fortified solid meals when infants get between the ages of six and twelve months. However, according to the current study, only 39.4% (N = 129) of the respondents said they never introduced semisolid food to their infant within the first six months. This information is available in Table 4.
Brushing is an essential part of good oral hygiene habits. In the current study, 94.2% (N = 308) of the parents agreed that their child’s teeth needed to be brushed or cleaned. This result appears in Table 3. Similar results got found by Madhavan and Mathew [11], who found that 80% of respondents thought brushing their teeth was necessary to prevent pediatric caries. Similar results are evident in a study conducted in 2007 by Gansky, Slayton, and Featherstone [12], who concluded that it is the parents’ and caregivers’ civic and moral duty to provide the best preventative management for young kids. Many of those surveyed in the current study had adequate knowledge of how nutrition affects oral health and thought that sugary snacks cause caries.
In the prenatal and infant phase, anticipatory guidance is still crucial. Shajahan, et al. [13] suggest that anticipatory guidance should evaluate any developmental or growth issues the parents should become aware of or that call for an appointment with the child’s doctor. The findings of Dhull, et al. [14] reveal when providing advice to parents concerning their kid’s fluoride exposure—which entails drinking optimally-fluoridated water, flossing with the right amount of fluoridated dental floss, and needing expert topical fluoride applications—the assessment of dental risk ought to be taken into account. 51.7% of participants in the current investigation (N = 169) disagree that children should see a dentist before age two. Table 3 contains this information. It conveys to the reader the importance of learning about oral hygiene.
Parents and other non-dental professionals can successfully include preventative dental procedures in caring for their children. Based on the results of the earlier research by Madhavan and Mathew [11] and Hancock, Schofield, and Zinn [8], parents in this study exhibited a consistent understanding of the significance of fluoride in preventing the development of dental caries. When asked how much toothpaste they use to brush their kids’ teeth, 29.4% (N = 96) mentioned a smear, 49.8% (N = 163) mentioned using a pea-sized amount, 16.5% (N = 54) mentioned using a whole brush length, and 4.3% (N = 14) mentioned not using any at all. This information is available in Table 4. Society can undoubtedly reduce the rate of pediatric dental caries and ensure healthy children with good smiles by remaining vigilant about prevention.
It is essential to maximize fluoride exposure for all children. Kadali, et al. [15] point out that anticipatory guidance over the infant period should also include education on brushing and flossing, dietary counseling about sugar consumption, a schedule for periodic dental examinations, and knowledge of nonnutritive routines that, if continued, may cause flaring decay in the upper jaw incisor teeth, a noticeable bite, and an inner mouth crossbite. Yildiz and Arikan [16] suggest counseling on safety and avoidance of orofacial damage should cover topics including playthings, pacifiers, automobile seats, electrical cables, and wounds sustained in accidents when starting to walk. In the current study, 75.5% of participants (N = 247) concur that frequent pacifier use may interfere with a child’s ability to develop their teeth normally (Table 3).
Some microbial organisms in a person’s mouth are responsible for tooth decay. Söderling and Pienihäkkinen [17] reveal evidence of downward transmission of Mutans Streptococci (MS) between mother and child. Furthermore, Aldhaher [3] contends that the risk of colonization of the newborn increases with maternal salivary concentrations. In addition to maternal salivary concentrations, baby colonization can get affected by the mother’s brushing and flossing habits, periodontal disease, frequent consumption of snacks, and socioeconomic position [17]. In the current study, 34.3% (N = 112) of children’s parents believed that bacteria spread by sharing eating utensils causing tooth decay. One can see this in Table 3.
To lower their risk of developing caries and manage caries by removing the point of infection and reducing the early baby inoculation, parents who suffer from elevated cariogenic microbial counts ought to seek professional dental care. According to the current study, parents are not aware that bacteria that cause tooth decay might spread downward. When asked if they bite food every time into small pieces before giving it to their child, 48.6% of respondents (N = 159) replied yes. 39.4% (N = 129) indicated they occasionally bite food into small pieces before serving it to their kids, compared to 9.5% (N = 31), who said they do so regularly. Only 2.5% (N = 8) of respondents claimed never to partake in the practice. This information is available in Table 4.
Each time parents express their desire to take action or make changes and their upbeat outlook, the better it improves children’s dental health. According to the findings of a prior study by Shah and Dave [18], 60% of the parents disagreed that nighttime bottling or breastfeeding caused tooth decay since they were ignorant of their harmful oral practices that may culminate in oral disorders. In the current study, 55% of respondents (N = 180) agreed that nighttime bottling or breastfeeding leads to tooth decay, while 45% of respondents (N = 147) disagreed. This information is available in Table 3 above. Burgette and Chi [4] explain that preschool environments lay the groundwork for oral health and usage patterns that continue into adulthood. Mothers, in particular, should be reminded that they serve as exemplars for their kids and get prompted to change their kid’s dental hygiene habits.
It is necessary to prevent cavities from an early age. Indira, et al. [19] suggest baby dental decay is a complex, dynamic, bacterially caused illness that causes phasic breakdown and remineralization of the hard tissues of the tooth. Acidogenic-aciduric strains of bacteria, such as Lactobacillus species, are traditional microbiological risk factors for baby dental caries [9]. In the current study, 88.1% (N = 288) agree that sugar is present in most food and beverages for children. This information is available in Table 2. Depending on the extent and frequency of contamination, dental cavities could be vertically transferred from parent to kid via salivary contact [10]. Infant dental caries bear a negative burden on kids’ and families’ enjoyment of life and place a needless monetary and health strain on society. The findings above explain why 96.9% (N = 317) of the respondents in the current study point out that they can make a difference in my kids’ oral health.
The limited number of samples and the localization of this investigation prevents the extrapolation of the findings. In assessing which measures will be most successful in changing parents’ behavior concerning newborn oral health care, research examining the same topic needs to get undertaken on larger samples from several demographics [20-26].
Parents’ awareness of maintaining an infant’s dental wellness was insufficient. Medical professionals must pass on relevant and correct information on toddler oral hygiene, using breastfeeding bottles at night, the importance of brushing teeth, and routine dental appointments. Essentially, medical professionals are the initial ones to interact with expecting and new moms. Creating and implementing extensive, long-term initiatives for expecting mothers’ wellness promotion and awareness of oral/ dental health is an important goal. The field of dentistry needs to broaden its strategy for infant/toddler cavities risk evaluation and management to encompass general dental offices plus medical care professionals to combat this expanding epidemic.
Declaration of interest
This research has not encountered conflicts of interest, and there hasn’t been any significant funding that would have affected the results of this investigation. The research has taken all necessary precautions to preserve the intellectual property connected to this task and guarantee no intellectual-property-related barriers to publishing, including the release date. The research was approved by the scientific research center at Psmmc.
The researcher appreciates the opportunity to have worked on this project with each person. The researcher would like to thank the parents who participated in this investigation for showing kindness in their cooperation and active involvement.
- Committee on Nutrition. American Academy of Pediatrics: The use and misuse of fruit juice in pediatrics. Pediatrics. 2001 May;107(5):1210-3. doi: 10.1542/peds.107.5.1210. PMID: 11331711.
- American Dental Association Council on Scientific Affairs. Fluoride toothpaste use for young children. J Am Dent Assoc. 2014 Feb;145(2):190-1. doi: 10.14219/jada.2013.47. Erratum in: J Am Dent Assoc. 2014 Mar;145(3):236. PMID: 24487611.
- Aldhaher ZA. Mutans Streptococci Count and Salivary Histatin 5 Level concerning Early Childhood Caries. Medico-Legal Update. 2021; 21(2).
- Burgette JM, Chi DL. Behavioral and Social Determinants of Oral Health in Children With Special Health Care Needs. Pediatrics. 2021 Aug;148(2):e2021050886. doi: 10.1542/peds.2021-050886. Epub 2021 Jul 21. PMID: 34290132.
- Cunha RF, Pugliesi DM, Garcia LD, Murata SS. Systemic and local teething disturbances: prevalence in a clinic for infants. J Dent Child (Chic). 2004 Jan-Apr;71(1):24-6. PMID: 15272651.
- Dagon N, Ratson T, Peretz B, Blumer S. Maternal Knowledge of Oral Health of Children Aged 1-4 Years. J Clin Pediatr Dent. 2019;43(2):116-120. doi: 10.17796/1053-4625-43.2.8. Epub 2019 Feb 7. PMID: 30730803.
- Dahlan R, Bohlouli B, Salami B, Saltaji H, Amin M. Parental acculturation and oral health of children among immigrants. J Public Health Dent. 2022 Sep;82(4):426-436. doi: 10.1111/jphd.12481. Epub 2021 Oct 21. PMID: 34672365.
- Hancock S, Schofield G, Zinn C. Healthy Food, Healthy Teeth: A Formative Study to Assess Knowledge of Foods for Oral Health in Children and Adults. Nutrients. 2022 Jul 21;14(14):2984. doi: 10.3390/nu14142984. PMID: 35889941; PMCID: PMC9319718.
- Ramos-Gomez FJ. A model for community-based pediatric oral heath: implementation of an infant oral care program. Int J Dent. 2014;2014:156821. doi: 10.1155/2014/156821. Epub 2014 Jan 23. PMID: 24587803; PMCID: PMC3920860.
- Wahyuni F, Rustina Y, Efendi D. Oral care prevents late-onset sepsis in risk. preterm infants. 2020.
- Madhavan S, Mathew MG. Assessment of the knowledge, attitude, and awareness among dental students about the prevention of dental caries in pediatric patients. Drug Invention Today. 2019; 11(8).
- Ramos-Gomez FJ, Crall J, Gansky SA, Slayton RL, Featherstone JD. Caries risk assessment appropriate for the age 1 visit (infants and toddlers). J Calif Dent Assoc. 2007 Oct;35(10):687-702. PMID: 18044377.
- Shajahan T, Harshitha K, Bhat SS, Hegde KS, Bhat VS. Poster 19: Infant Oral Care-An Eyeopener For Nurses. Dental Poster Journal. 2020; 9(2): 1-3.
- Dhull KS, Indira MD, Dhull RS, Sawhney B. Infant oral health care: An invaluable clinical intervention. Indian Journal of Dental Sciences. 2016; 8(3): 183.
- Kadali LM, Mopagar V, Shetty S, Shetty S, Chaudhari VKS. Infant Oral Health Care Concerning Education of Mothers--Part 2. Journal of Evolution of Medical and Dental Sciences. 2021; 10(31): 2538-2543.
- Yildiz A, Arikan D. The effects of giving pacifiers to premature infants and making them listen to lullabies on their transition period for total oral feeding and sucking success. J Clin Nurs. 2012 Mar;21(5-6):644-56. doi: 10.1111/j.1365-2702.2010.03634.x. Epub 2011 Jun 13. PMID: 21668549.
- Söderling E, Pienihäkkinen K. Effects of xylitol and erythritol consumption on mutans streptococci and the oral microbiota: a systematic review. Acta Odontol Scand. 2020 Nov;78(8):599-608. doi: 10.1080/00016357.2020.1788721. Epub 2020 Jul 7. PMID: 32633595.
- Shah SS, Dave BH. The Co-relation of Salivary Streptococcus Mutans' Count between Mothers and their Neonates within Two Days of Life: An Ex Vivo Microbial Study. Journal of Pediatrics, Perinatology, and Child Health. 2022; 6(1): 104-114.
- Indira MD, Dhull KS, Nandlal B. Knowledge, Attitude and Practice toward Infant Oral Healthcare among the Pediatricians of Mysore: A Questionnaire Survey. Int J Clin Pediatr Dent. 2015 Sep-Dec;8(3):211-4. doi: 10.5005/jp-journals-10005-1315. Epub 2015 Sep 11. PMID: 26604540; PMCID: PMC4647042.
- Douglass JM, Li Y, Tinanoff N. Association of mutans streptococci between caregivers and their children. Pediatr Dent. 2008 Sep-Oct;30(5):375-87. PMID: 18942596.
- Davey AL, Rogers AH. Multiple types of the bacterium Streptococcus mutans in the human mouth and their intra-family transmission. Arch Oral Biol. 1984;29(6):453-60. doi: 10.1016/0003-9969(84)90026-8. PMID: 6589988.
- Feldens CA, Faraco IM, Ottoni AB, Feldens EG, Vítolo MR. Teething symptoms in the first year of life and associated factors: a cohort study. J Clin Pediatr Dent. 2010 Spring;34(3):201-6. PMID: 20578655.
- Milgrom PM, Huebner CE, Ly KA. Fluoridated toothpaste and the prevention of early childhood caries: a failure to meet the needs of our young. J Am Dent Assoc. 2009 Jun;140(6):628, 630-1. doi: 10.14219/jada.archive.2009.0235. PMID: 19491152; PMCID: PMC2746689.
- Tinanoff N, Kanellis MJ, Vargas CM. Current understanding of the epidemiology mechanisms, and prevention of dental caries in preschool children. Pediatr Dent. 2002 Nov-Dec;24(6):543-51. PMID: 12528947.
- van Loveren C, Buijs JF, ten Cate JM. Similarity of bacteriocin activity profiles of mutans streptococci within the family when the children acquire the strains after the age of 5. Caries Res. 2000 Nov-Dec;34(6):481-5. doi: 10.1159/000016627. PMID: 11093022.
- Wake M, Hesketh K, Allen M. Parent beliefs about infant teething: a survey of Australian parents. J Paediatr Child Health. 1999 Oct;35(5):446-9. doi: 10.1046/j.1440-1754.1999.355395.x. PMID: 10571756.